
Hypercoagulable states — MCQs

A 21-year-old woman comes to the physician because of a 1-day history of right leg pain. The pain is worse while walking and improves when resting. Eight months ago, she was diagnosed with a pulmonary embolism and was started on warfarin. Anticoagulant therapy was discontinued two months ago. Her mother had systemic lupus erythematosus. On examination, her right calf is diffusely erythematous, swollen, and tender. Cardiopulmonary examination shows no abnormalities. On duplex ultrasonography, the right popliteal vein is not compressible. Laboratory studies show an elevated serum level of D-dimer and insensitivity to activated protein C. Further evaluation of this patient is most likely to show which of the following?
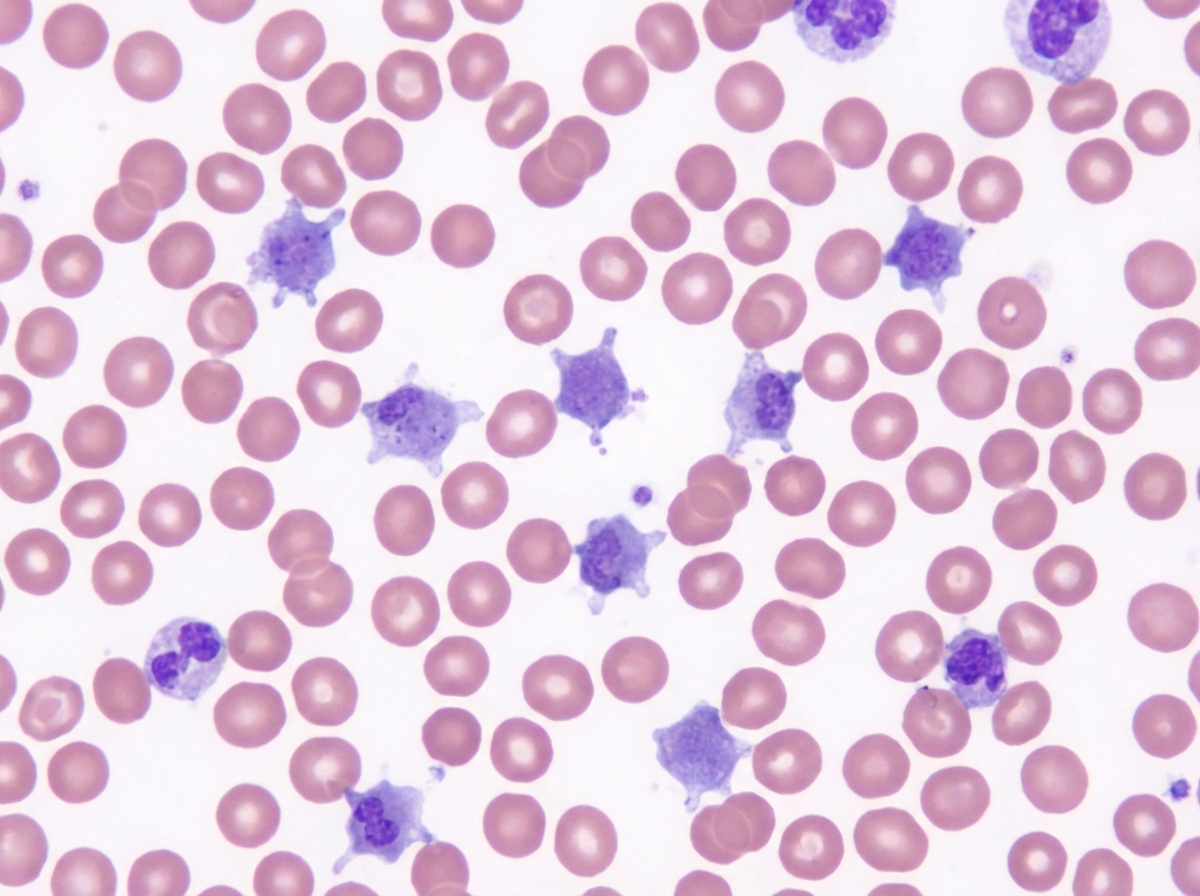
A 3-week-old boy is brought to the pediatrician by his parents for a circumcision. The circumcision was uncomplicated; however, after a few hours, the diaper contained blood, and the bleeding has not subsided. A complete blood count was ordered, which was significant for a platelet count of 70,000/mm3. On peripheral blood smear, the following was noted (figure A). The prothrombin time was 12 seconds, partial thromboplastin time was 32 seconds, and bleeding time was 13 minutes. On platelet aggregation studies, there was no response with ristocetin. This result was not corrected with the addition of normal plasma. There was a normal aggregation response with the addition of ADP. Which of the following is most likely true of this patient's underlying disease?
A 29-year-old woman comes to the office with her husband because she has had 4 spontaneous abortions. Regarding her medical history, she was diagnosed with systemic lupus erythematosus 9 years ago, had a stroke 3 years ago, and was diagnosed with deep vein thrombosis in the same year. She has no relevant family history. Her vital signs include: heart rate 78/min, respiratory rate 14/min, temperature 37.5°C (99.5°F), and blood pressure 120/85 mm Hg. The physical examination is unremarkable. The complete blood count results are as follows: Hemoglobin 12.9 g/dL Hematocrit 40% Leukocyte count 8,500/mm3 Neutrophils 55% Bands 2% Eosinophils 1% Basophils 0% Lymphocytes 29% Monocytes 2% Platelet count 422,000/mm3 Her coagulation test results are as follows: Partial thromboplastin time (activated) 50.9 s Prothrombin time 13.0 s A VDRL test is done, and the result is positive. Mixing studies are performed, and they fail to correct aPTT. What is the most likely cause in this patient?
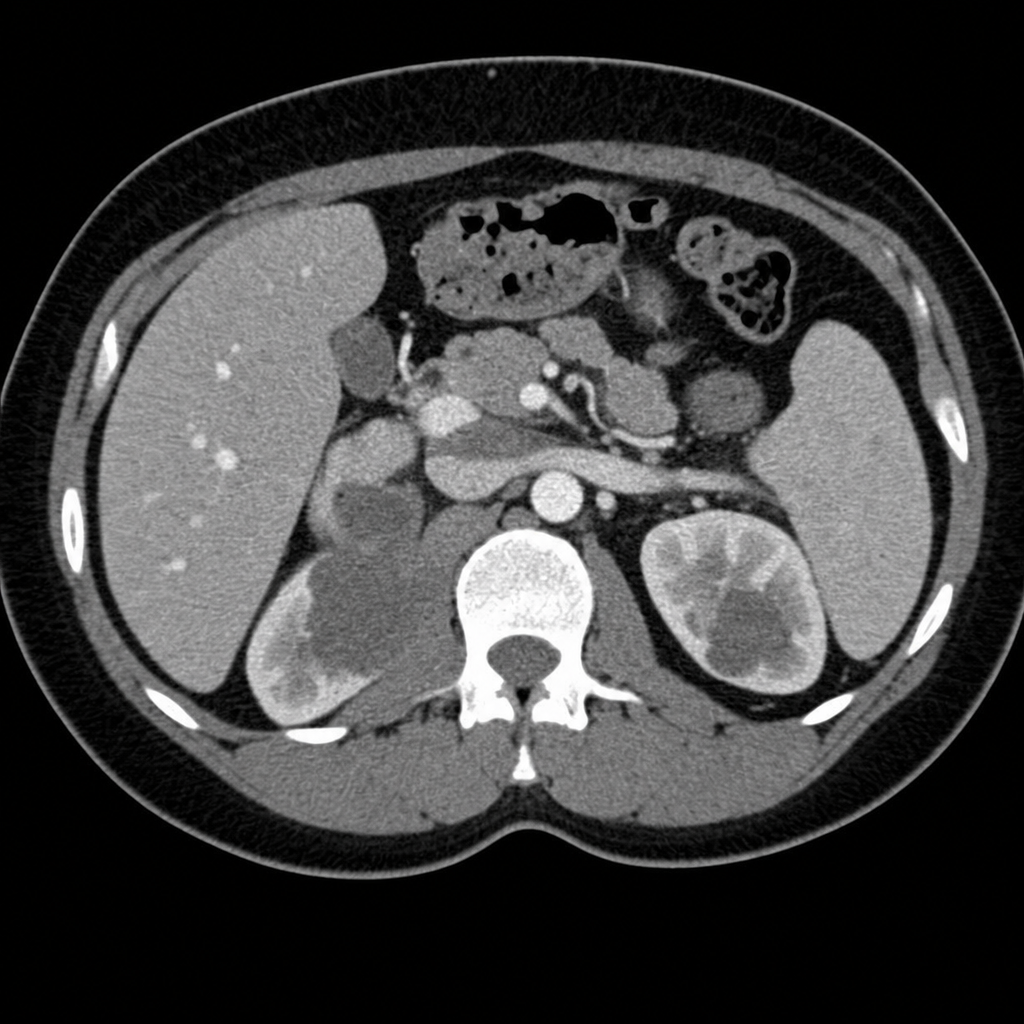
A 30-year-old woman presents to her primary care provider with blood in her urine and pain in her left flank. She has a 5-year history of polycystic ovarian syndrome managed with oral contraceptives and metformin. She is single and is not sexually active and denies a history of kidney stones or abdominal trauma. She has a 15-pack-year smoking history but denies the use of other substances. Her family history is significant for fatal lung cancer in her father at age 50, who also smoked, and recently diagnosed bladder cancer in her 45-year-old brother, who never smoked. On review of systems, she denies weight loss, fever, fatigue, paresthesia, increased pain with urination, or excessive bleeding or easy bruising. She is admitted to the hospital for a workup and observation. Her vital signs and physical exam are within normal limits. A urine pregnancy test is negative. PT is 14 sec and PTT is 20 sec. The rest of the laboratory results including von Willebrand factor activity and lupus anticoagulant panel are pending. A CT angiogram is ordered and is shown in the picture. What is indicated at this time to prevent a potential sequela of this patient’s condition?
A 12-year-old boy is brought by his mother to the emergency room because of a swollen, hot, and tender knee that he sustained after falling on his way home. He has never had a swollen joint before; however, he has had frequent nosebleeds throughout his life. His mother is worried because they live with her parents who are currently on blood thinners. Every morning she puts the blood thinner pill in the boy's grandfather's milk and was concerned that she may have switched it this morning. Family history reveals a number of uncles who have had bleeding disorders; however, the mother does not know the exact disorder suffered by these relatives. A hematologic panel reveals the following findings: Bleeding time: Increased Prothrombin time: 12 seconds Partial thromboplastin time (PTT): 55 seconds PTT after factor mixing study: 37 seconds Which of the following most likely explains the abnormal partial thromboplastin time in this patient?
A 35-year-old woman presents to her primary care physician for recurrent deep venous thrombosis (DVT) of her left lower extremity. She is a vegetarian and often struggles to maintain an adequate intake of non-animal based protein. She currently smokes 1 pack of cigarettes per day, drinks a glass of wine per day, and currently denies any illicit drug use, although she endorses a history of heroin use (injection). Her past medical history is significant for 4 prior admissions for lower extremity swelling and pain that resulted in diagnoses of deep venous thrombosis. Her vital signs include: temperature, 36.7°C (98.0°F); blood pressure, 126/74 mm Hg; heart rate, 87/min; and respiratory rate, 16/min. On physical examination, her pulses are bounding, the patient's complexion is pale, breath sounds are clear, and heart sounds are normal. The spleen is mildly enlarged. She is admitted for DVT treatment and a full hypercoagulability workup. Which of the following is the best initial management for this patient?
A 57-year-old immigrant from Nigeria presents to the emergency department for sudden, severe pain and swelling in her lower extremity. She was at a rehabilitation hospital when her symptoms became apparent. The patient has a past medical history of obesity, diabetes, bipolar disorder, and tonic-clonic seizures. Her current medications include metformin, insulin, lisinopril, and valproic acid. The patient is a prominent IV drug and alcohol user who has presented to the ED many times for intoxication. On physical exam you note anasarca and asymmetric lower extremity swelling. Based on the results of a doppler ultrasound of her swollen lower extremity, heparin is started. The patient is then transferred to the general medicine floor for continued management. Laboratory studies are shown below. Serum: Na+: 137 mEq/L K+: 5.5 mEq/L Cl-: 100 mEq/L HCO3-: 24 mEq/L Urea nitrogen: 22 mg/dL Ca2+: 5.7 mg/dL Creatinine: 1.7 mg/dL Glucose: 70 mg/dL The patient's presentation includes generalized edema (anasarca) along with laboratory abnormalities. What is the most likely underlying diagnosis that explains her overall clinical presentation?
A 61-year-old man presents to the emergency room with a painful, swollen left leg. He states that his symptoms began that morning after a long flight from Australia. He denies shortness of breath, chest pain, or cough. On review of systems, he notes that he has been constipated recently and had several episodes of bright red blood per rectum. He has not noticed any weight loss, fevers, or night sweats. He has a past medical history of a deep vein thrombosis 4 years ago during a hospitalization for community acquired pneumonia and was treated with warfarin for 3 months afterward. He also has chronic hepatitis C from previous intravenous drug use. The patient has a 30 pack-year smoking history and has never had a colonoscopy. His father is 84-years-old and has chronic kidney disease from diabetes, and his mother passed away from a massive pulmonary embolus when pregnant with his younger sister. In the emergency room, his temperature is 98.7°F (37.1°C), blood pressure is 142/85 mm/Hg, pulse is 79/min, and respirations are 14/min. On exam, he is in no acute distress. His left calf is larger in caliber than the right calf which is red and tender to palpation. Dorsiflexion of the foot worsens the pain. His abdomen is soft, nontender, and nondistended without hepatomegaly. The remainder of the physical exam is unremarkable. Labs are shown below: Hemoglobin: 13.0 g/dL Leukocyte count: 6,000/mm^3 Platelets: 160,000/mm^3 Aspartate aminotransferase: 15 U/L Alanine aminotransferase: 19 U/L Alkaline phosphatase: 81 IU/L Hepatitis C antibody: reactive Hepatitis C titer: 0 copies/mL Which of the following is the most likely cause of this patient’s condition?
A 24-year-old woman comes to the physician because of pain and swelling of her left leg over the past 24 hours. The pain is worse while walking and improves when resting. Seven months ago, she was diagnosed with a pulmonary embolism and was started on warfarin. Anticoagulant therapy was discontinued 1 month ago. Her sister has systemic lupus erythematosus. The patient does not smoke. She currently takes no medications. Her temperature is 37.8°C (100°F), pulse is 78/min, and blood pressure is 123/72 mm Hg. On physical examination, the left calf is diffusely erythematous, swollen, and tender. Dorsal flexion of the left foot elicits pain. Cardiopulmonary examination shows no abnormalities. On duplex ultrasonography, the left popliteal vein is not compressible. Laboratory studies show an elevated serum concentration of D-dimer and insensitivity to activated protein C. Further examination is most likely to show which of the following?
A 48-year-old man comes to the emergency department because of sudden right flank pain that began 3 hours ago. He also noticed blood in his urine. Over the past two weeks, he has developed progressive lower extremity swelling and a 4-kg (9-lb) weight gain. Examination shows bilateral 2+ pitting edema of the lower extremities. Urinalysis with dipstick shows 4+ protein, positive glucose, and multiple red cell and fatty casts. Abdominal CT shows a large right kidney with abundant collateral vessels and a filling defect in the right renal vein. Which of the following is the most likely underlying cause of this patient's symptoms?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app