
Anemia of chronic disease — MCQs

A 78-year-old man presents with fatigue and exertional dyspnea. The patient says that symptoms onset gradually 4 weeks ago and have not improved. He denies any history of anemia or nutritional deficiency. Past medical history is significant for ST-elevation myocardial infarction 6 months ago, status post coronary artery bypass graft, complicated by recurrent hemodynamically unstable ventricular tachycardia. Current medications are rosuvastatin, aspirin, and amiodarone. His blood pressure is 100/70 mm Hg, the pulse is 71/min, the temperature is 36.5°C (97.7°F), and the respiratory rate is 16/min. On physical examination, patient appears lethargic and tired. Skin is dry and coarse, and there is generalized pitting edema present. A complete blood count (CBC) and a peripheral blood smear show evidence of normochromic, normocytic anemia. Additional laboratory tests reveal decreased serum level of iron, decreased TIBC (total iron-binding capacity) and increased serum level of ferritin. Which of the following is the most likely etiology of the anemia in this patient?
A 39-year-old woman presents with progressive weakness, exercise intolerance, and occasional dizziness for the past 3 months. Past medical history is unremarkable. She reports an 18-pack-year smoking history and drinks alcohol rarely. Her vital signs include: temperature 36.6°C (97.8°F), blood pressure 139/82 mm Hg, pulse 98/min. Physical examination is unremarkable. Her laboratory results are significant for the following: Hemoglobin 9.2 g/dL Erythrocyte count 2.1 million/mm3 Mean corpuscular volume (MCV) 88 μm3 Mean corpuscular hemoglobin (MCH) 32 pg/cell Leukocyte count 7,500/mm3 Which of the following is the best next step in the management of this patient’s condition?
A 55-year-old woman presents with fatigue. She says her symptoms are present throughout the day and gradually started 4 months ago. Her past medical history is significant for rheumatoid arthritis–treated with methotrexate, and diabetes mellitus type 2–treated with metformin. The patient is afebrile, and her vital signs are within normal limits. A physical examination reveals pallor of the mucous membranes. Initial laboratory tests show hemoglobin of 7.9 g/dL, hematocrit of 22%, and mean corpuscular volume of 79 fL. Which of the following is the best next diagnostic step in this patient?
A 63-year-old man with a history of stage 4 chronic kidney disease (CKD) has started to develop refractory anemia. He denies any personal history of blood clots in his past, but he says that his mother has also had to be treated for deep venous thromboembolism in the past. His past medical history is significant for diabetes mellitus type 2, hypertension, non-seminomatous testicular cancer, and hypercholesterolemia. He currently smokes 1 pack of cigarettes per day, drinks a glass of wine per day, and he currently denies any illicit drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 87/min, and respiratory rate 17/min. On physical examination, the pulses are bounding, the complexion is pale, but breath sounds remain clear. Oxygen saturation was initially 91% on room air, with a new oxygen requirement of 2 L by nasal cannula. His primary care physician refers him to a hematologist, who is considering initiating the erythropoietin-stimulating agent (ESA), darbepoetin. Which of the following is true regarding the use of ESA?
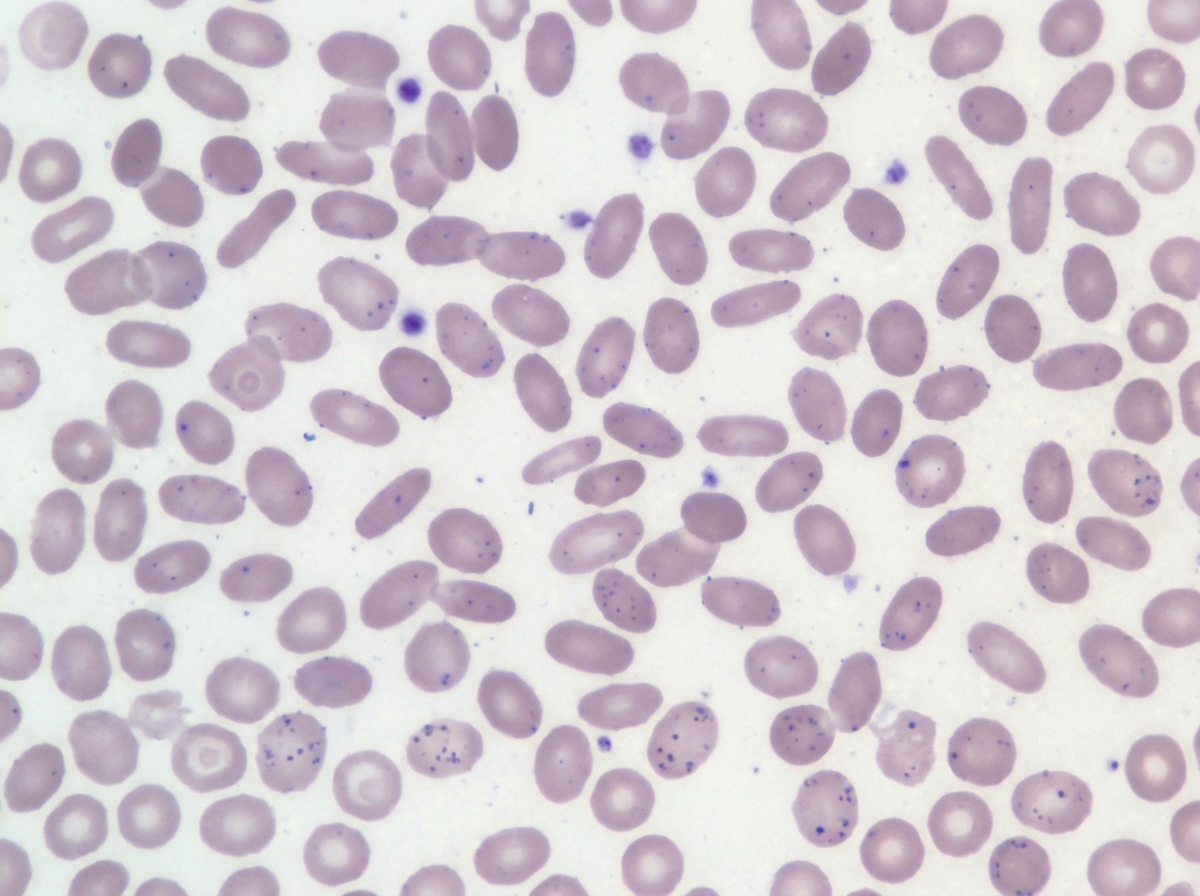
A 7-year-old boy is brought to the pediatrician by his parents for concern of general fatigue and recurrent abdominal pain. You learn that his medical history is otherwise unremarkable and that these symptoms started about 3 months ago after they moved to a different house. Based on clinical suspicion labs are obtained that reveal a microcytic anemia with high-normal levels of ferritin. Examination of a peripheral blood smear shows findings that are demonstrated in the figure provided. Which of the following is the most likely mechanism responsible for the anemia in this patient?
A 61-year-old man with a history of stage IIIa lung adenocarcinoma that has been treated with wedge resection and chemotherapy presents to the primary care clinic. He is largely asymptomatic, but he demonstrates a persistent microcytic anemia despite iron supplementation. Colonoscopy performed 3 years earlier was unremarkable. His past medical history is significant for diabetes mellitus type II, hypertension, acute lymphoblastic leukemia as a child, and hypercholesterolemia. He currently smokes 1 pack of cigarettes per day, drinks a glass of pinot grigio per day, and currently denies any illicit drug use. His vital signs include: temperature, 36.7°C (98.0°F); blood pressure, 126/74 mm Hg; heart rate, 87/min; and respiratory rate, 17/min. On physical examination, his pulses are bounding, complexion is pale, but breath sounds remain clear. Oxygen saturation was initially 91% on room air, with a new oxygen requirement of 2 L by nasal cannula. Which of the following lab values would suggest anemia of chronic disease as the underlying etiology?
A 72-year-old woman comes to the physician because of a 1-month history of progressive fatigue and shortness of breath. Physical examination shows generalized pallor. Laboratory studies show: Hemoglobin 5.8 g/dL Hematocrit 17% Mean corpuscular volume 86 μm3 Leukocyte count 6,200/mm3 with a normal differential Platelet count 240,000/mm3 A bone marrow aspirate shows an absence of erythroid precursor cells. This patient’s condition is most likely associated with which of the following?
A 76-year-old woman comes in for a routine checkup with her doctor. She is concerned that she feels tired most days and has difficulty doing her household chores. She complains that she gets fatigued and breathless with mild exertion. Past medical history is significant for diabetes mellitus, chronic kidney disease from prolonged elevated blood sugar, and primary biliary cirrhosis. Medications include lisinopril, insulin, and metformin. Family medicine is noncontributory. She drinks one beer every day. Today, she has a heart rate of 98/min, respiratory rate of 17/min, blood pressure of 110/65 mm Hg, and a temperature of 37.0°C (98.6°F). General examination shows that she is pale and haggard looking. She has a heartbeat with a regular rate and rhythm and her lungs are clear to auscultation bilaterally. A complete blood count (CBC) is as follows: Leukocyte count: 12,000/mm3 Red blood cell count: 3.1 million/mm3 Hemoglobin: 11.0 g/dL MCV: 85 fL MCH: 27 pg/cell Platelet count: 450,000/mm3 Fecal occult blood test is negative. What is the most likely cause of her anemia?
A 25-year-old woman is being evaluated due to complaint of fatigue and voiding pink urine. The laboratory results are as follows: Hb 6.7 Red blood cell count 3.0 x 1012/L Leukocyte count 5,000/mm3 Platelets 170 x 109/L Reticulocyte count 6% Hematocrit 32% The physician thinks that the patient is suffering from an acquired mutation in hematopoietic stem cells, which is confirmed by flow cytometry analysis that revealed these cells are CD 55 and CD 59 negative. However, the physician is interested in knowing the corrected reticulocyte count before starting the patient on eculizumab. What value does the physician find after calculating the corrected reticulocyte count?
A 68-year-old woman comes to the physician because of increasing heartburn for the last few months. During this period, she has taken ranitidine several times a day without relief and has lost 10 kg (22 lbs). She has retrosternal pressure and burning with every meal. She has had heartburn for several years and took ranitidine as needed. She has hypertension. She has smoked one pack of cigarettes daily for the last 40 years and drinks one glass of wine occasionally. Other current medications include amlodipine and hydrochlorothiazide. She appears pale. Her height is 163 cm (5 ft 4 in), her weight is 75 kg (165 lbs), BMI is 27.5 kg/m2. Her temperature is 37.2°C (98.96°F), pulse is 78/min, and blood pressure is 135/80 mm Hg. Cardiovascular examination shows no abnormalities. Abdominal examination shows mild tenderness to palpation in the epigastric region. Bowel sounds are normal. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 10.2 g/dL Mean corpuscular volume 78 μm Mean corpuscular hemoglobin 23 pg/cell Leukocyte count 9,500/mm3 Platelet count 330,000/mm3 Serum Na+ 137 mEq/L K+ 3.8 mEq/L Cl- 100 mEq/L HCO3- 25 mEq/L Creatinine 1.2 mg/dL Lactate dehydrogenase 260 U/L Alanine aminotransferase 18 U/L Aspartate aminotransferase 15 U/L Lipase (N < 280 U/L) 40 U/L Troponin I (N < 0.1 ng/mL) 0.029 ng/mL An ECG shows normal sinus rhythm without ST-T changes. Which of the following is the most appropriate next step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app