
Valvular heart disease and heart failure — MCQs

A 68-year-old man comes to the emergency department because of a 1-week history of difficulty breathing. He has had recurrent palpitations over the past 2 years. During this time, he has also had several episodes of anxiety despite no change in his daily life. He has occasional sharp chest pain localized to the left upper sternal border. He has no abdominal pain or leg swelling. Two years ago, he had streptococcal pharyngitis, which was promptly treated with a 10-day course of penicillin. He has never traveled outside of the country. His temperature is 36.5°C (97.7°F), pulse is 82/min, and blood pressure is 140/85 mm Hg. Physical examination shows a 3/6 holosystolic murmur that is loudest at the apex and radiates to the axilla with a mid-systolic click. Bilateral fine crackles are heard on lung auscultation. Which of the following is the most likely cause of this patient's symptoms?
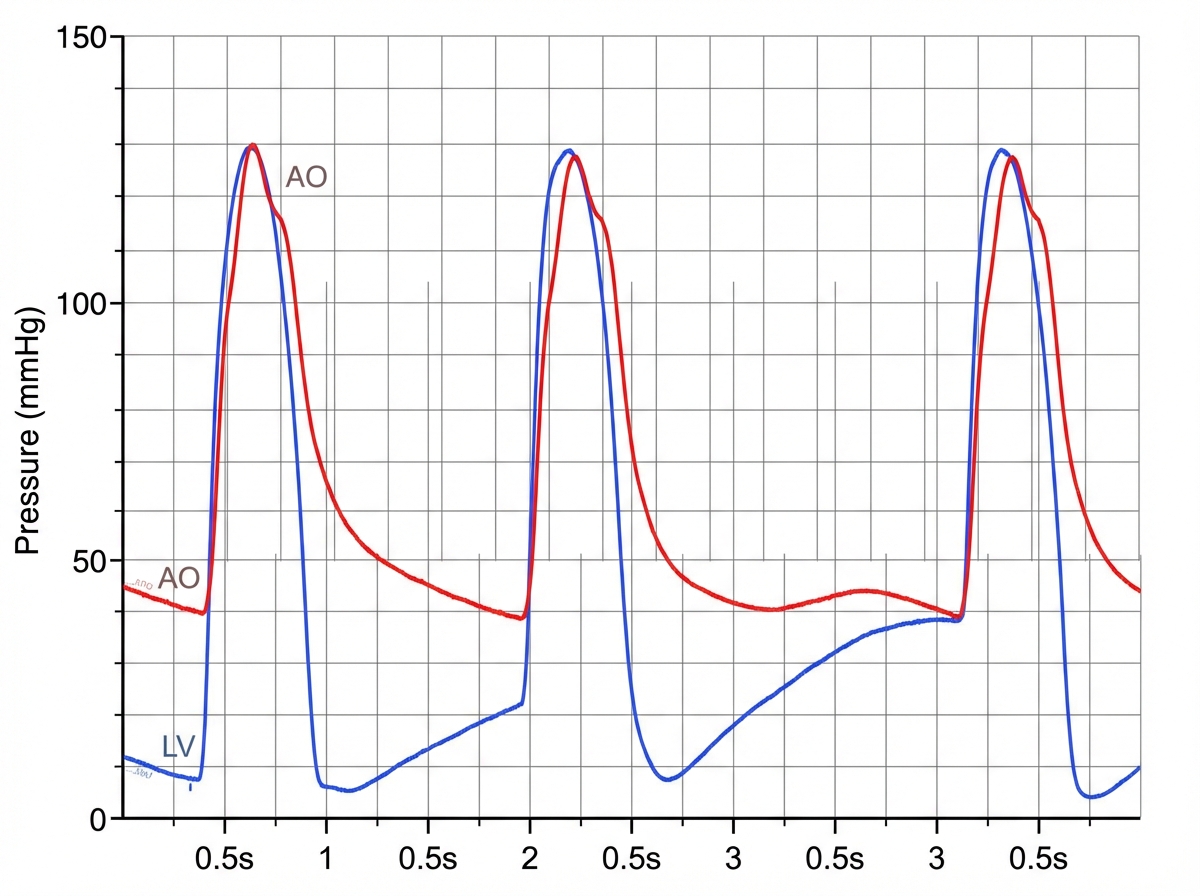
A 31-year-old man comes to the physician because of a 5-day history of fever, chills, and dyspnea. His temperature is 38.9°C (102°F) and pulse is 90/min. Cardiac examination shows a murmur. In addition to other measures, cardiac catheterization is performed. A graph showing the results of the catheterization is shown. This patient most likely has which of the following valvular heart defects?
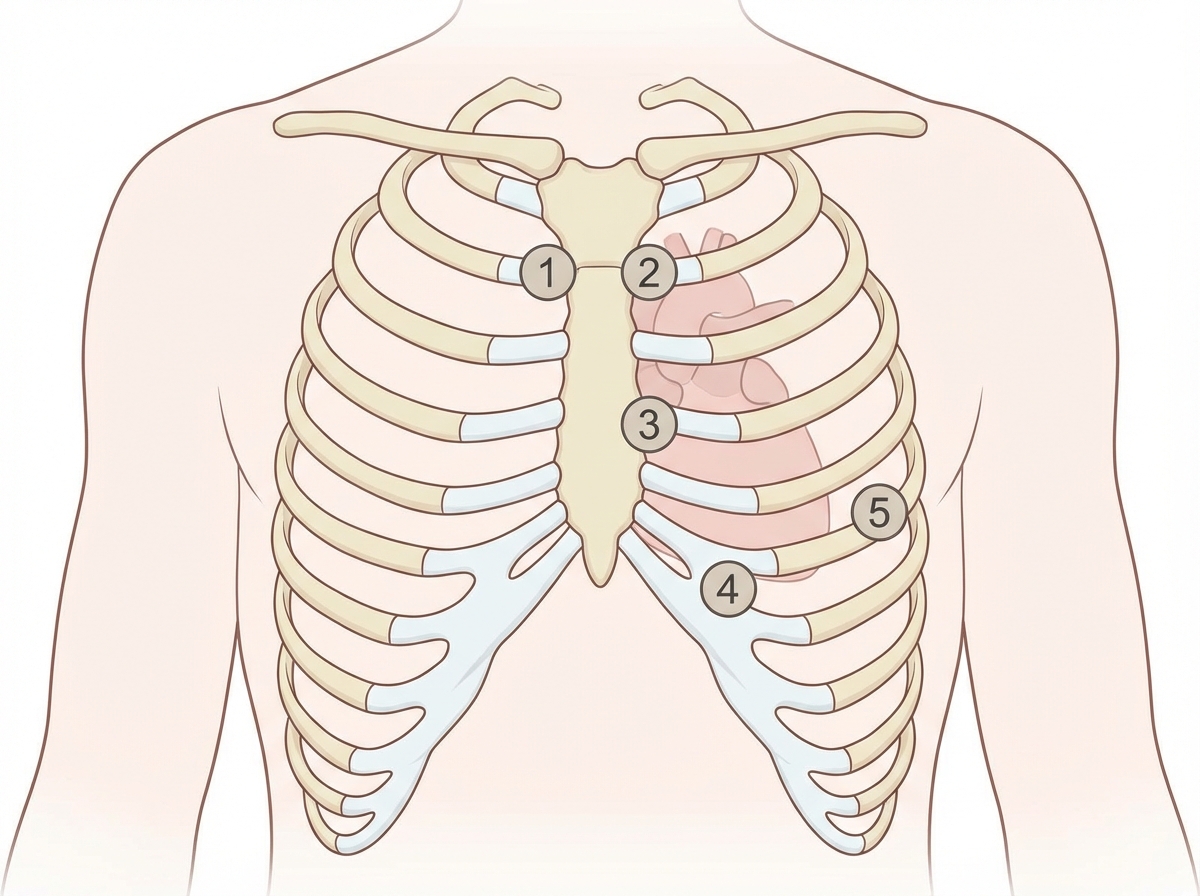
A 27-year-old woman, who recently immigrated from Bangladesh, presents to her primary care physician to discuss birth control. During a review of her past medical history, she reports that as a child she had a recurrent sore throat and fever followed by swollen and aching hip and knee joints. These symptoms returned every season and were never treated but went away on their own only to return with the next typhoon season. When asked about any current complaints, the patient says that she sometimes has shortness of breath and palpitations that do not last long. A physical exam is performed. In which of the auscultation sites will a murmur most likely be heard in this patient?
A 27-year-old woman with a history of a "heart murmur since childhood" presents following a series of syncopal episodes over the past several months. She also complains of worsening fatigue over this time period, and notes that her lips have begun to take on a bluish tinge, for which she has been using a brighter shade of lipstick. You do a careful examination, and detect a right ventricular heave, clubbing of the fingers, and 2+ pitting edema bilaterally to the shins. Despite your patient insisting that every doctor she has ever seen has commented on her murmur, you do not hear one. Transthoracic echocardiography would most likely detect which of the following?
A 72-year-old man who was involved in a traffic collision is brought to the emergency room by the ambulance service. He was in shock and comatose at the time of presentation. On examination, the heart rate is 60/min, and the blood pressure is 70/40 mm Hg. The patient dies, despite resuscitative efforts. Autopsy reveals multiple internal hemorrhages and other evidence of ischemic damage affecting the lungs, kidneys, and brain. The patient’s heart shows evidence of gross anomaly similar to the picture. While acute hypovolemia is the likely cause of the ischemic changes seen in the lungs, kidneys, and brain, which of the following best explains the gross anomaly of his heart?

A 50-year-old female presents with a holosystolic murmur heard best over the apex, radiating to the axilla. She has no signs of pulmonary hypertension or edema. What best explains her lack of symptoms?
A 64-year-old woman with a history of rheumatic fever presents to her primary care clinician complaining of excessive fatigue with walking and difficulty lying flat. She had no prior physical limitations, but recently has been unable to walk more than 3 blocks without needing to stop and rest. Her cardiac exam is notable for a late diastolic murmur heard best at the apex in the left lateral decubitus position with no radiation. What is the most likely diagnosis?
A 34-year-old male is brought to the emergency department. He has prior hospitalizations for opiate overdoses, but today presents with fever, chills, rigors and malaise. On physical exam vitals are temperature: 100.5 deg F (38.1 deg C), pulse is 105/min, blood pressure is 135/60 mmHg, and respirations are 22/min. You note the following findings on the patient's hands (Figures A and B). You note that as the patient is seated, his head bobs with each successive heart beat. Which of the following findings is most likely present in this patient?

An 85-year-old man presents to his primary care provider after feeling "lightheaded." He said he helped his wife in the garden for the first time, but that while moving some bags of soil he felt like he was going to faint. He had a big breakfast of oatmeal and eggs prior to working in the garden. He has no significant past medical history and takes a baby aspirin daily. Physical exam reveals an elderly, well-nourished, well-built man with no evidence of cyanosis or tachypnea. Vital signs show normal temperature, BP 150/70, HR 80, RR 18. Cardiac exam reveals crescendo-decrescendo systolic murmur. What is the most likely cause of this patient's diagnosis?
A 36-year-old man presents to his primary care physician because of shortness of breath. He is an office worker who has a mostly sedentary lifestyle; however, he has noticed that recently he feels tired and short of breath when going on long walks with his wife. He also has had a hacking cough that seems to linger, though he attributes this to an upper respiratory tract infection he had 2 months ago. He has diabetes that is well-controlled on metformin and has smoked 1 pack per day for 20 years. Physical exam reveals a large chested man with wheezing bilaterally and mild swelling in his legs and abdomen. The cause of this patient's abdominal and lower extremity swelling is most likely due to which of the following processes?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app