
Heart failure — MCQs

On this page
A 71-year-old woman with a past medical history of type 2 diabetes, hypercholesterolemia, and hypertension was admitted to the hospital 8 hours ago with substernal chest pain for management of acute non-ST-elevated myocardial infarction (NSTEMI). The ECG findings noted by ST-depressions and T-wave inversions on anterolateral leads, which is also accompanied by elevated cardiac enzymes. Upon diagnosis, management with inhaled oxygen therapy, beta-blockers and aspirin, and low-molecular-weight heparin therapy were initiated, and she was placed on bed rest with continuous electrocardiographic monitoring. Since admission, she required 2 doses of sublingual nitroglycerin for recurrent angina, and the repeat troponin levels continued to rise. Given her risk factors, plans were made for early coronary angiography. The telemetry nurse calls the on-call physician because of her concern with the patient's mild confusion and increasing need for supplemental oxygen. At bedside evaluation, The vital signs include: heart rate 122/min, blood pressure 89/40 mm Hg, and the pulse oximetry is 91% on 6L of oxygen by nasal cannula. The telemetry and a repeat ECG show sinus tachycardia. She is breathing rapidly, appears confused, and complains of shortness of breath. On physical exam, the skin is cool and clammy and appears pale and dull. She has diffuse bilateral pulmonary crackles, and an S3 gallop is noted on chest auscultation with no new murmurs. She has jugular venous distention to the jaw-line, rapid and faint radial pulses, and 1+ dependent edema. She is immediately transferred to the intensive care unit for respiratory support and precautions for airway security. The bedside sonography shows abnormal hypodynamic anterior wall movement and an ejection fraction of 20%, but no evidence of mitral regurgitation or ventricular shunt. The chest X-ray demonstrates cephalization of pulmonary veins and pulmonary edema. What is the most appropriate next step in the stabilization of this patient?
A 57-year-old woman with type 2 diabetes mellitus comes to the physician for a follow-up examination. She previously had been compliant with her diet and medication but has had a 5-kg (11-lb) weight gain since the last visit 6 months ago. She reports that she often misses doses of her metformin. Her hemoglobin A1c is 9.8%. Which of the following is the most appropriate course of action?
A 55-year-old man presents with a bilateral lower leg edema. The patient reports it developed gradually over the past 4 months. The edema is worse in the evening and improves after sleeping at night or napping during the day. There are no associated pain or sensitivity changes. The patient also notes dyspnea on usual exertion such as working at his garden. The patient has a history of a STEMI myocardial infarction 9 months ago treated with thrombolysis with an unremarkable postprocedural course. His current medications include atorvastatin 10 mg, aspirin 81 mg, and metoprolol 50 mg daily. He works as a barber at a barbershop, has a 16-pack-year history of smoking, and consumes alcohol in moderation. The vital signs include: blood pressure 130/80 mm Hg, heart rate 63/min, respiratory rate 14/min, and temperature 36.8℃ (98.2℉). The lungs are clear to auscultation. Cardiac examination shows dubious S3 and a soft grade 1/6 systolic murmur best heard at the apex of the heart. Abdominal examination reveals hepatic margin 1 cm below the costal margin. There is a 2+ bilateral pitting lower leg edema. The skin over the edema is pale with no signs of any lesions. There is no facial or flank edema. The thyroid gland is not enlarged. Which of the following tests is most likely to reveal the cause of the patient’s symptoms?
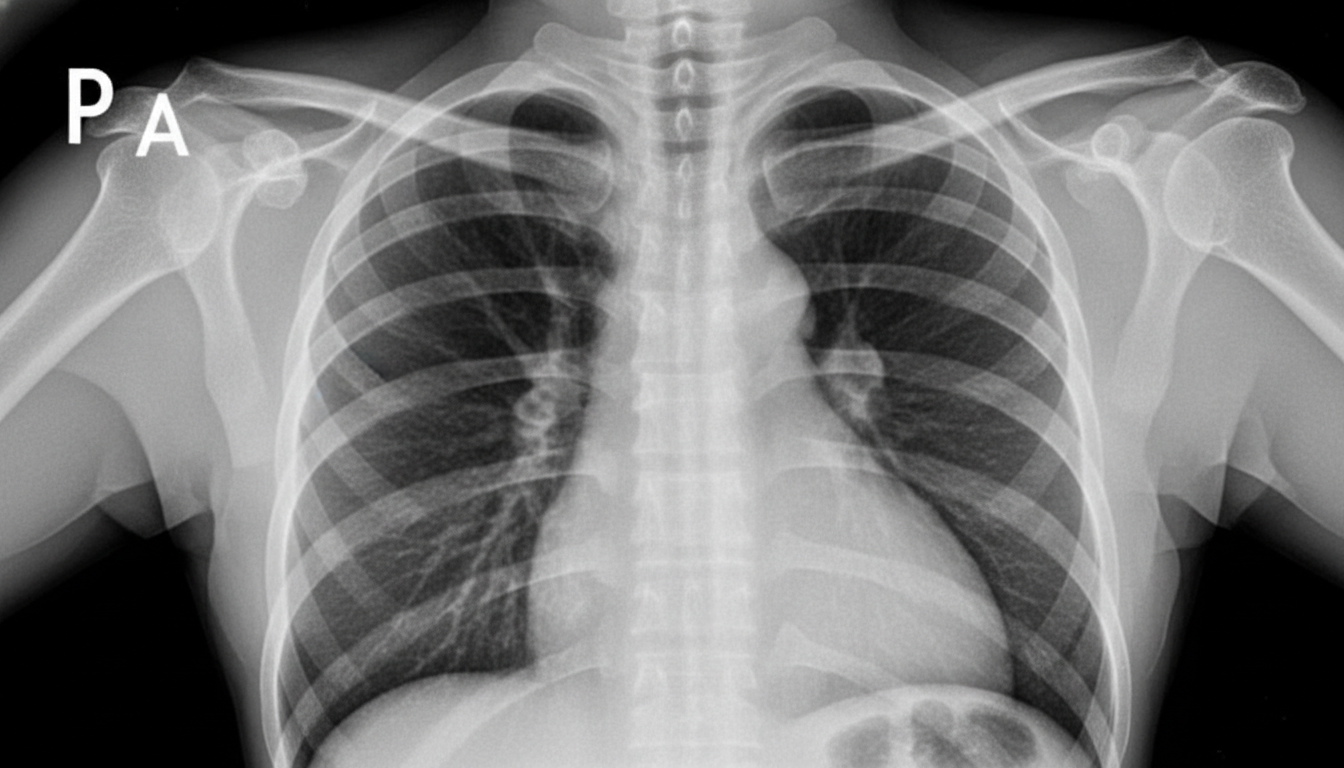
A 75-year-old over-weight gentleman with a long history of uncontrolled hypertension, diabetes, smoking and obesity is presenting to his primary care physician with a chief complaint of increased difficulty climbing stairs and the need to sleep propped up by an increasing number of pillows at night. On physical examination the patient has an extra heart sound just before S1 heard best over the cardiac apex and clear lung fields. The EKG and chest x-ray are attached (Figures A and B respectively). What is the largest contributor to this patient's symptoms?
A 78-year-old man presents to the clinic complaining of shortness of breath at rest and with exertion. He also complains of difficulty breathing while lying down. He also is concerned because he startles from sleep and feels like he is choking. These symptoms have been bothering him for the last several weeks and they are getting worse. He has been afebrile with no known sick contacts. 6 months ago, he had an acute myocardial infarction from which he recovered and until recently had felt well. He has a history of hyperlipidemia for which he takes atorvastatin. His temperature is 37.0°C (98.6°F), the pulse is 85/min, the respiratory rate is 14/min, and the blood pressure is 110/75 mm Hg. On physical examination, his heart has a regular rate and rhythm. He has bilateral crackles in both lungs. An echocardiogram is performed and shows a left ventricular ejection fraction of 33%. What medication should be started?
A 38-year-old woman comes to the physician because of an 8-week history of shortness of breath and dull chest pain. She has a history of antiphospholipid syndrome. Physical examination shows jugular venous distention. Right heart catheterization shows a mean pulmonary arterial pressure of 30 mm Hg and a pulmonary capillary wedge pressure of 10 mm Hg. Further evaluation is most likely to show which of the following?
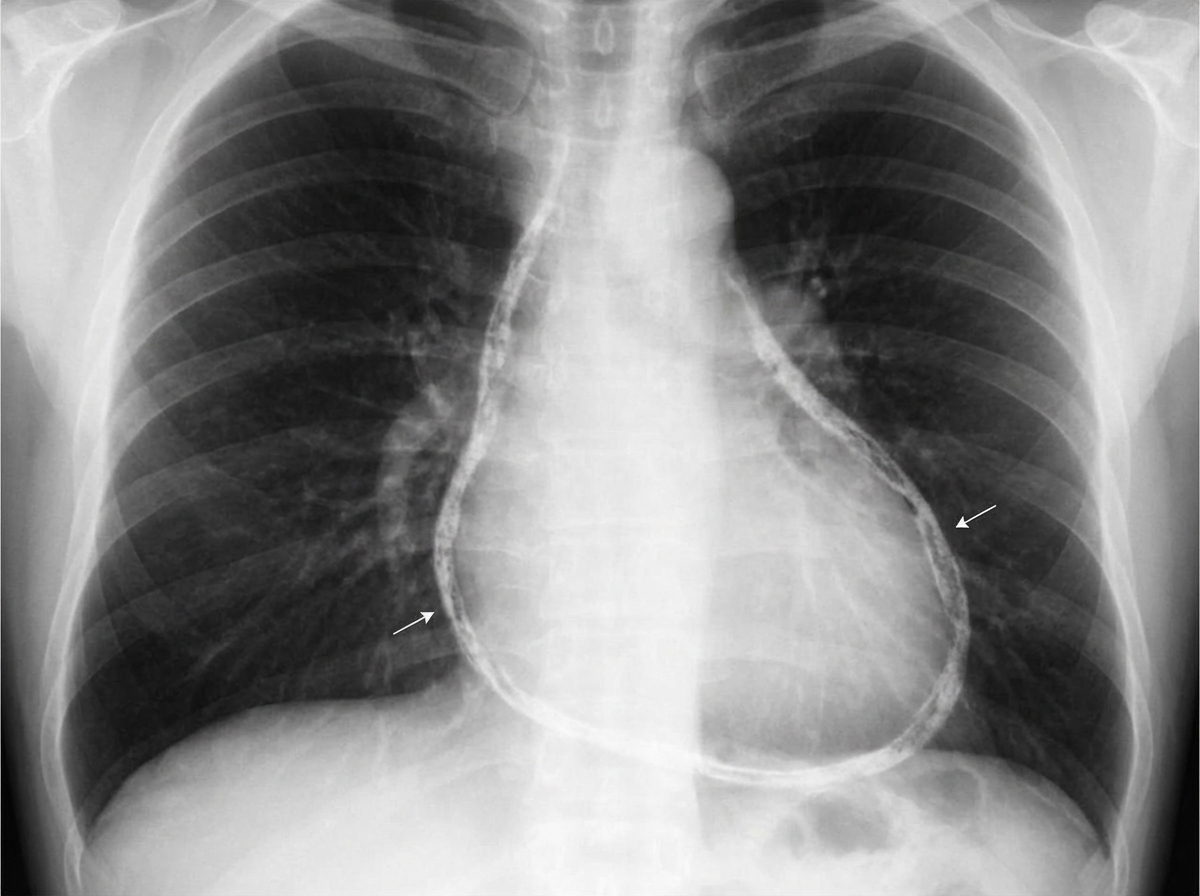
A 64-year-old man who recently immigrated to the United States from Haiti comes to the physician because of a 3-week history of progressively worsening exertional dyspnea and fatigue. For the past few days, he has also had difficulty lying flat due to trouble breathing. Over the past year, he has had intermittent fever, night sweats, and cough but he has not been seen by a physician for evaluation of these symptoms. His temperature is 37.8°C (100°F). An x-ray of the chest is shown. Further evaluation of this patient is most likely to show which of the following findings?
A 43-year-old man comes to the physician because of increasing shortness of breath for 1 month. He has been using two pillows at night but frequently wakes up feeling as if he is choking. Five months ago, he underwent surgery for creation of an arteriovenous fistula in his left upper arm. He has hypertension and chronic kidney disease due to reflux nephropathy. He receives hemodialysis three times a week. His current medications are enalapril, vitamin D3, erythropoietin, sevelamer, and atorvastatin. His temperature is 37.1°C (98.8°F), respirations are 22/min, pulse is 103/min and bounding, and blood pressure is 106/58 mm Hg. Examination of the lower extremities shows bilateral pitting pedal edema. There is jugular venous distention. A prominent thrill is heard over the brachiocephalic arteriovenous fistula. There are crackles heard at both lung bases. Cardiac examination shows an S3 gallop. The abdomen is soft and nontender. Which of the following is the most likely cause of this patient's symptoms?
A 75-year-old woman presents to her physician with a cough and shortness of breath. She says that cough gets worse at night and her shortness of breath occurs with moderate exertion or when lying flat. She says these symptoms have been getting worse over the last 6 months. She mentions that she has to use 3 pillows while sleeping in order to relieve her symptoms. She denies any chest pain, chest tightness, or palpitations. Past medical history is significant for hypertension and diabetes mellitus type 2. Her medications are amiloride, glyburide, and metformin. Family history is significant for her father who also suffered diabetes mellitus type 2 before his death at 90 years old. The patient says she drinks alcohol occasionally but denies any smoking history. Her blood pressure is 130/95 mm Hg, temperature is 36.5°C (97.7°F), and heart rate is 100/min. On physical examination, she has a sustained apical impulse, a normal S1 and S2, and a loud S4 without murmurs. There are bilateral crackles present bilaterally. A chest radiograph shows a mildly enlarged cardiac silhouette. A transesophageal echocardiogram is performed and shows a normal left ventricular ejection fraction. Which of the following myocardial changes is most likely present in this patient?
A 45-year-old woman presents to the physician with a 6-month history of progressive shortness of breath. She now has to stop to rest three or four times whenever she climbs the stairs to her apartment on the third floor. She reports chronic, nonproductive cough and wheezing, for which she uses ipratropium inhalers. She has a 25 pack-year smoking history. On examination, the blood pressure is 130/80 mm Hg, the pulse rate is 95/min, the temperature is 36.6°C (97.8°F), and the respiratory rate is 26/min. Chest auscultation reveals bilateral crepitations. Cardiac auscultation reveals normal S1 and S2 without murmurs or added sounds. Arterial blood gas analysis shows: pH 7.36 (reference: 7.35–7.45) HCO3- 32 mEq/L (reference 22–28 mEq/L) Pco2 48 mm Hg (reference: 33–45 mm Hg) Po2 63 mm Hg (reference: 75–105 mm Hg) O2 saturation 91% (reference: 94–99%) Which of the following would you expect to find in this patient?
Practice by Chapter
Classification of heart failure (HFrEF vs HFpEF)
Practice Questions
Heart failure pathophysiology
Practice Questions
Acute decompensated heart failure
Practice Questions
Chronic heart failure management
Practice Questions
Guideline-directed medical therapy
Practice Questions
Device therapy for heart failure
Practice Questions
Cardiomyopathies
Practice Questions
Valvular heart disease and heart failure
Practice Questions
Right heart failure
Practice Questions
Pulmonary hypertension
Practice Questions
Cardio-renal syndrome
Practice Questions
Advanced heart failure and transplantation
Practice Questions
Quality measures in heart failure
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app