
Heart failure — MCQs

On this page
A 82-year-old man who is currently being managed by the internal medicine service agrees to be examined by medical students as part of their training in physical examination. He is visited by a small group of medical students under the instruction of a preceptor and allows the students to make observations. They find that he has bibasilar crackles that are most prominent during inspiration as well as some wheezing. Furthermore, he coughs up some sputum during the exam, and this sputum is found to have a rust color. He does not report any pain and no skin findings are seen. Which of the following conditions best explains this patient's physical exam findings?
Background and Methods: Aldosterone is important in the pathophysiology of heart failure. In a double-blind study, we enrolled 1,663 patients who had severe heart failure, a left ventricular ejection fraction of no more than 35 percent, and were being treated with an angiotensin-converting-enzyme inhibitor, a loop diuretic, and in most cases digoxin. A total of 822 patients were randomly assigned to receive 25 mg of spironolactone daily and 841 to receive placebo. The primary endpoint was death from all causes. Results: The trial was discontinued early, after a mean follow-up period of 24 months, because an interim analysis determined that spironolactone was efficacious. There were 386 deaths in the placebo group (46%) and 284 in the spironolactone group (35%; relative risk of death, 0.70; 95% confidence interval, 0.60 to 0.82; p<0.001). This 30 percent reduction in the risk of death among patients in the spironolactone group was attributed to a lower risk of both death from progressive heart failure and sudden death from cardiac causes. The frequency of hospitalization for worsening heart failure was 35% lower in the spironolactone group than in the placebo group (relative risk of hospitalization, 0.65; 95% confidence interval, 0.54 to 0.77; p<0.001). In addition, patients who received spironolactone had a significant improvement in the symptoms of heart failure, as assessed on the basis of the New York Heart Association functional class (p<0.001). Gynecomastia was reported in 10% of men who were treated with spironolactone, as compared with 1% of men in the placebo group (p<0.001). The incidence of serious hyperkalemia was minimal in both groups of patients. Which of the following statements represents the most accurate interpretation of the results from the aforementioned clinical trial?
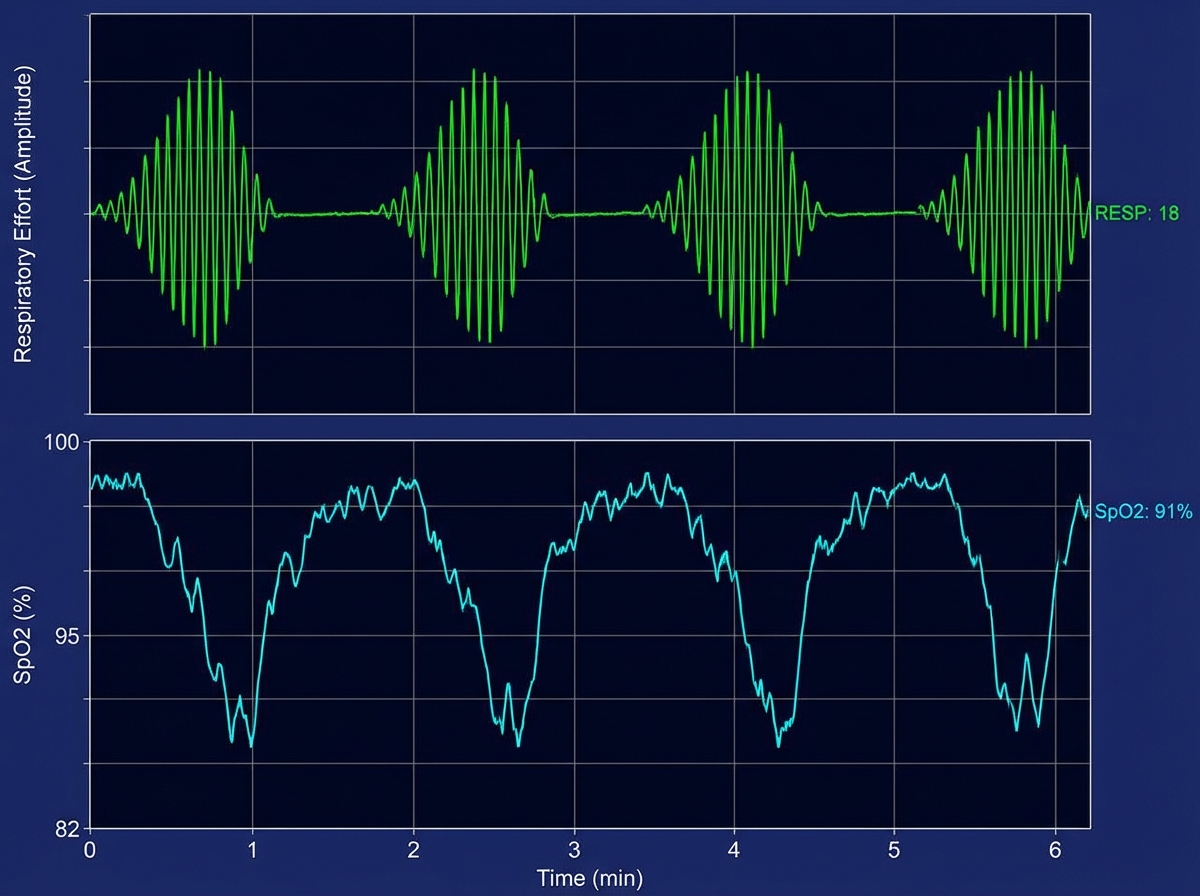
A 66-year-old man is brought to the emergency department because of shortness of breath and confusion. His pulse is 98/min, and blood pressure is 109/73 mm Hg. He is oriented to person but not time or place. A graph of his breathing pattern and oxygen saturation is shown. Which of the following additional findings is most likely present in this patient?
A 14-year-old girl is brought to the physician for a follow-up examination. She has had frequent falls over the past two years. During the past six months, the patient has been unable to walk or stand without assistance and she now uses a wheelchair. Her mother was diagnosed with a vestibular schwannoma at age 52. Her vital signs are within normal limits. Her speech is slow and unclear. Neurological examination shows nystagmus in both eyes. Her gait is wide-based with irregular and uneven steps. Her proprioception and vibration sense are absent. Muscle strength is decreased especially in the lower extremities. Deep tendon reflexes are 1+ bilaterally. The remainder of the examination shows kyphoscoliosis and foot inversion with hammer toes. This patient is most likely to die from which of the following complications?
A 72-year-old man presents with shortness of breath and right-sided chest pain. Physical exam reveals decreased breath sounds and dull percussion at the right lung base. Chest X-ray reveals a right-sided pleural effusion. A thoracentesis was performed, removing 450 mL of light pink fluid. Pleural fluid analysis reveals: Pleural fluid to serum protein ratio: 0.35 Pleural fluid to serum LDH ratio: 0.49 Lactate dehydrogenase (LDH): 105 IU (serum LDH Reference: 100–190) Which of the following disorders is most likely in this patient?
A 45-year-old man with a 5-year history of worsening shortness of breath and cough comes to the physician for a follow-up examination. He has never smoked. His pulse is 75/min, blood pressure is 130/65 mm Hg, and respirations are 25/min. Examination shows an increased anteroposterior diameter of the chest. Diminished breath sounds and wheezing are heard on auscultation of the chest. An x-ray of the chest shows widened intercostal spaces, a flattened diaphragm, and basilar-predominant bullous changes of the lungs. This patient is at increased risk for which of the following complications?
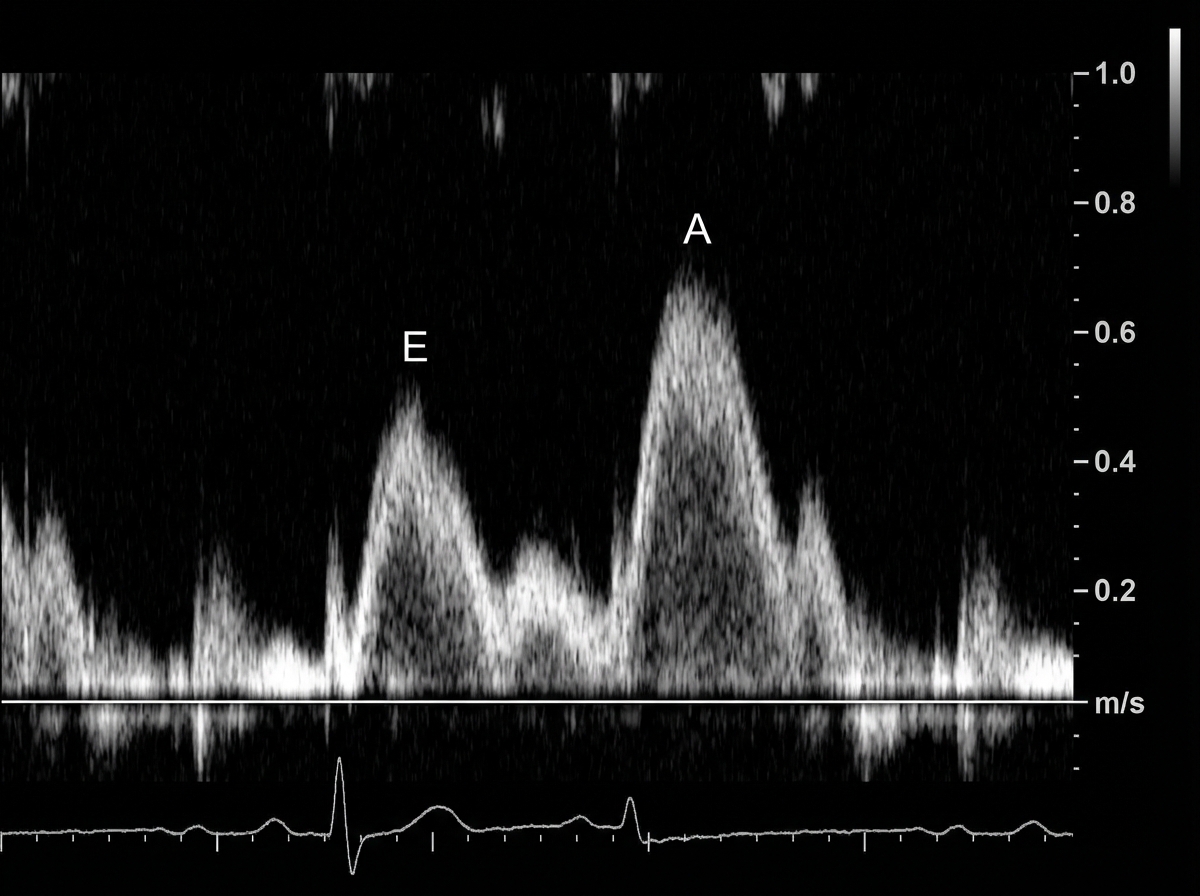
A 49-year-old man presents to his physician complaining of weakness and fatigue. Lab work reveals an elevated transferrin saturation of 72% and a serum ferritin of 1,850 ng/mL. On exam, you note significant peripheral edema. Transthoracic echocardiogram is performed and reveals a preserved ejection fraction with impaired diastolic relaxation. A representative still image is shown in Image A. Which of the following is likely the cause of this patient's symptoms?
A 48-year-old man comes to the physician because of a 3-month history of worsening shortness of breath and cough productive of frothy, whitish sputum. One year ago, he had a similar episode lasting 6 months. He has smoked a pack of cigarettes daily for 25 years. Physical examination shows bluish discoloration of the tongue and lips. Scattered expiratory wheezing and rhonchi are heard throughout both lung fields. Further evaluation of this patient is most likely to show which of the following findings?
A 81-year-old man presents to his primary care physician with a 4-month history of shortness of breath. He says that he has slowly lost the ability to do things due to fatigue and now gets winded after walking around the house. He also says that his cough has been getting worse and seems to be producing more sputum. He has gained about 5 pounds over the last 6 months. His past medical history is significant for hypertension and diabetes. He has a 40 pack-year smoking history and drinks about 3 drinks per week. Physical exam reveals a cyanotic appearing man with 1+ edema in his legs bilaterally. He also has wheezing on lung auscultation with a prolonged expiratory phase. Which of the following would most likely be seen on a chest radiograph in this patient?
A 75-year-old man is brought to the emergency department for a 5-day-history of worsening dyspnea, orthopnea, and lower leg swelling. He has a history of hypertension, hyperlipidemia, non-alcoholic fatty liver disease, and myocardial infarction 10 years ago. Current medications include metoprolol, lisinopril, ethacrynic acid, eplerenone, and aspirin. He drinks 1 beer daily. He has a 30-pack-year smoking history. He is allergic to sulfonamides. His temperature is 37.0°C (98.6°F), his pulse is 120/min, and his blood pressure is 120/80 mm Hg. Physical examination reveals jugular venous distention and 3+ pitting edema in his lower legs. Crackles are heard at both lung bases. The point of maximal impulse is 2 cm to the left of the midclavicular line in the 6th intercostal space. Which of the following additional findings would be most strongly associated with increased mortality?
Practice by Chapter
Classification of heart failure (HFrEF vs HFpEF)
Practice Questions
Heart failure pathophysiology
Practice Questions
Acute decompensated heart failure
Practice Questions
Chronic heart failure management
Practice Questions
Guideline-directed medical therapy
Practice Questions
Device therapy for heart failure
Practice Questions
Cardiomyopathies
Practice Questions
Valvular heart disease and heart failure
Practice Questions
Right heart failure
Practice Questions
Pulmonary hypertension
Practice Questions
Cardio-renal syndrome
Practice Questions
Advanced heart failure and transplantation
Practice Questions
Quality measures in heart failure
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app