
Heart failure — MCQs

On this page
A 70-year-old male presents for an annual exam. His past medical history is notable for shortness of breath when he sleeps, and upon exertion. Recently he has experienced dyspnea and lower extremity edema that seems to be worsening. Both of these symptoms have resolved since he was started on several medications and instructed to weigh himself daily. Which of the following is most likely a component of his medical management?
A 70-year-old man comes to the physician because of a 6-month-history of worsening shortness of breath on exertion and bouts of coughing while sleeping. He has hypertension, hyperlipidemia, and type 2 diabetes mellitus. Current medications include lisinopril, simvastatin, and insulin. The patient appears tired but in no acute distress. His pulse is 70/min, blood pressure is 140/85 mm Hg, and respirations are 25/min. He has crackles over both lower lung fields and 2+ pitting edema of the lower extremities. An ECG shows T wave inversions in leads V1 to V4. Which of the following agents is most likely to improve the patient's long-term survival?
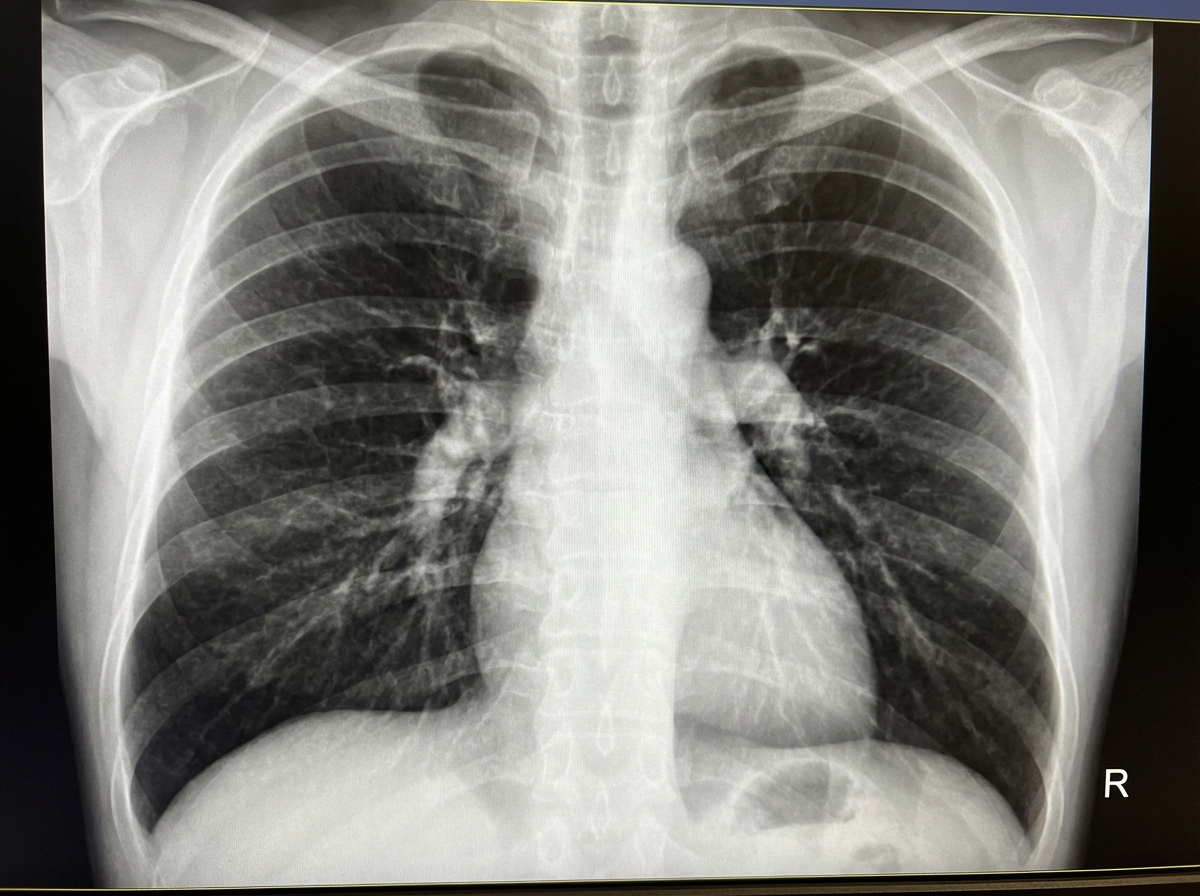
A 68-year-old man presents with shortness of breath, particularly when walking up stairs and when lying down to go to sleep at night. He also complains of a chronic cough and states that he now uses 2 extra pillows at night. The patient has a history of type 2 diabetes that is well-managed with metformin. He also takes Prozac for a long-standing history of depression. The patient has a 60-pack-year smoking history. He also has a history significant for alcohol abuse, but he quit cold turkey 15 years ago when his brother was killed in a drunk driving accident. Both he and his brother were adopted, and he does not know other members of his biological family. Despite repeated efforts of patient counseling, the patient is not interested in quitting smoking. The physical exam is significant for an obese male using accessory muscles of respiration. The vital signs include: temperature 36.8°C (98.2°F), heart rate 95/min, respiratory rate 16/min, and blood pressure 130/85 mm Hg. The oxygen saturation is 88% on room air. Additional physical exam findings include cyanotic lips, peripheral edema, hepatomegaly, and ascites. The cardiovascular exam is significant for an S3 heart sound and elevated JVP. The pulmonary exam is significant for expiratory wheezing, diffuse rhonchi, and hyperresonance on percussion. A bedside echocardiogram reveals a dilated right ventricle with preserved left ventricular ejection fraction (LVEF 60%), findings consistent with cor pulmonale rather than left-sided systolic heart failure. The laboratory test results are as follows: BUN 15 mg/dL pCO2 60 mm Hg Bicarbonate (HCO3) 32 mmol/L Creatinine 0.8 mg/dL Glucose 95 mg/dL Serum chloride 103 mmol/L Serum potassium 3.9 mEq/L Serum sodium 140 mEq/L Total calcium 2.3 mmol/L Hemoglobin 26 g/dL Bilirubin total 0.9 mg/dL Bilirubin indirect 0.4 mg/dL Iron 100 Ferritin 70 TIBC 300 The posterior-anterior chest X-ray is shown in the image. Which of the following interventions is indicated for decreasing the mortality of this patient?
A 64-year-old male with a history of coronary artery disease, hypertension, hyperlipidemia, and type II diabetes presents to his primary care physician with increasing shortness of breath and ankle swelling over the past month. Which of the following findings is more likely to be seen in left-sided heart failure and less likely to be seen in right-sided heart failure?
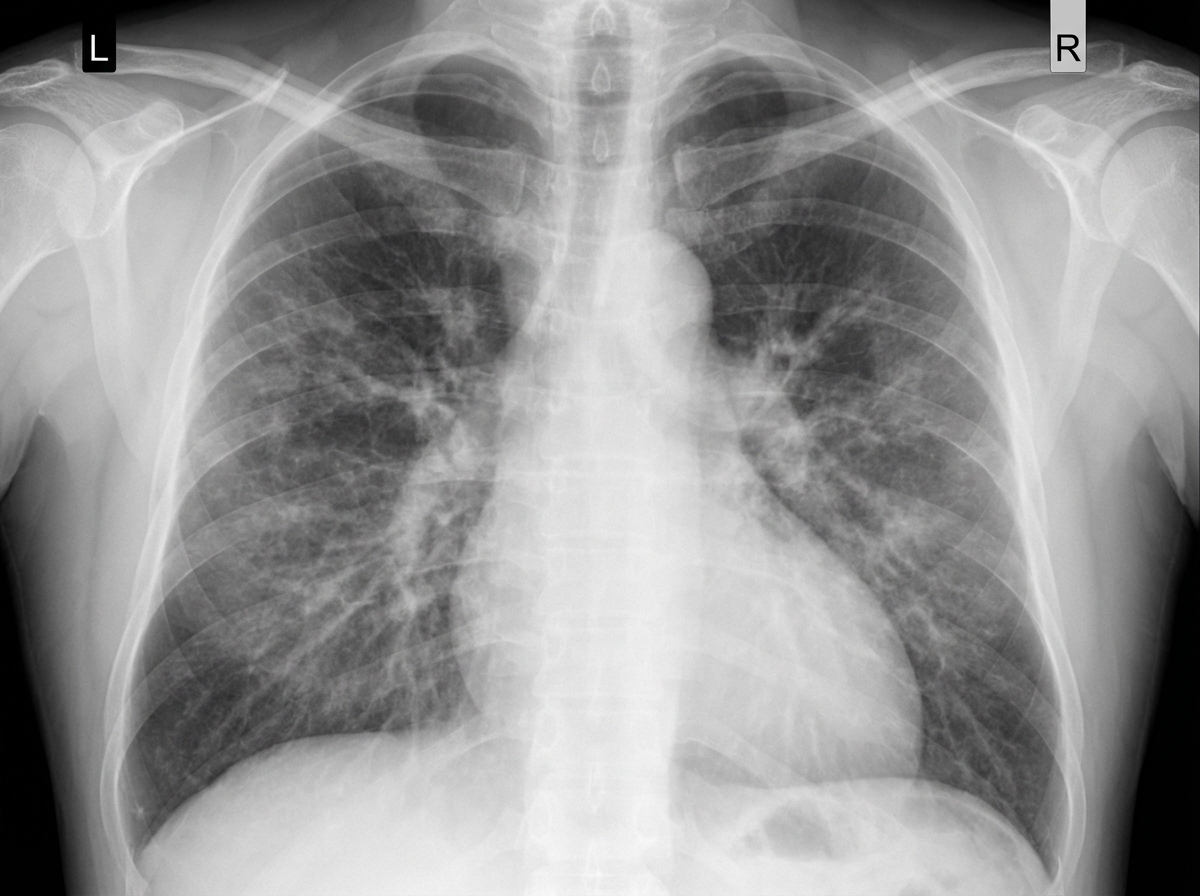
A 58-year-old man comes to the physician because of a 5-day history of progressively worsening shortness of breath and fatigue. He has smoked 1 pack of cigarettes daily for 30 years. His pulse is 96/min, respirations are 26/min, and blood pressure is 100/60 mm Hg. An x-ray of the chest is shown. Which of the following is the most likely cause of this patient's findings?
A 65-year-old male presents to your office complaining of worsening shortness of breath. He has experienced shortness of breath on and off for several years, but is noticing that it is increasingly more difficult. Upon examination, you note wheezing and cyanosis. You conduct pulmonary function tests, and find that the patient's FEV1/FVC ratio is markedly decreased. What is the most likely additional finding in this patient?
A 55-year-old man presents to the emergency department with shortness of breath and fatigue. His symptoms began insidiously and progressively worsened over the course of a month. He becomes short of breath when climbing the stairs or performing low-intensity exercises. He also needs to rest on multiple pillows in order to comfortably sleep. A few weeks ago he developed fever, malaise, and chest pain. Medical history is significant for hypertension, hypercholesterolemia, type II diabetes, and bariatric surgery performed 10 years ago. He is taking lisinopril, atorvastatin, and metformin. He drinks alcohol occasionally and does not smoke. He tried cocaine 3 days ago for the first time and has not used the illicit drug since. Physical exam is significant for bibasilar crackles, an S3 heart sound, and a laterally displaced cardiac apex. He has normal muscle tone throughout, 2+ reflexes, and an intact sensory exam. Which of the following is most likely the cause of this patient's symptoms?
A 56-year-old man presents to the emergency department with increasing shortness of breath and mild chest discomfort. One week ago he developed cold-like symptoms, including a mild fever, headache, and occasional night sweats. He noticed that he required 2 additional pillows in order to sleep comfortably. Approximately 1-2 nights ago, he was severely short of breath, causing him to awaken from sleep which frightened him. He reports gaining approximately 6 pounds over the course of the week without any significant alteration to his diet. He says that he feels short of breath after climbing 1 flight of stairs or walking less than 1 block. Previously, he was able to climb 4 flights of stairs and walk 6-7 blocks with mild shortness of breath. Medical history is significant for coronary artery disease (requiring a left anterior descending artery stent 5 years ago and dual antiplatelet therapy), heart failure with reduced ejection fraction, hypertension, hyperlipidemia, and type II diabetes. He drinks 2 alcoholic beverages daily and has smoked 1 pack of cigarettes daily for the past 35 years. His temperature is 98.6°F (37°C), blood pressure is 145/90 mmHg, pulse is 102/min, and respirations are 20/min. On physical exam, the patient has a positive hepatojugular reflex, a third heart sound, crackles in the lung bases, and pitting edema up to the mid-thigh bilaterally. Which of the following is the best next step in management?
A 64-year-old man with longstanding ischemic heart disease presents to the clinic with complaints of increasing exercise intolerance and easy fatigability for the past 2 weeks. He further states that he has been experiencing excessive daytime somnolence and shortness of breath with exertion. His wife adds that his shortness of breath is more in the recumbent position, and after approximately 2 hours of sleep, after which he suddenly wakes up suffocating and gasping for breath. This symptom is relieved after assuming an upright position for more than 30 minutes. The vital signs are as follows: heart rate, 126/min; respiratory rate, 16/min; temperature, 37.6°C (99.6°F); and blood pressure, 122/70 mm Hg. The physical examination reveals a S3 gallop on cardiac auscultation and positive hepatojugular reflux with distended neck veins. An electrocardiogram shows ischemic changes similar to ECG changes noted in the past. An echocardiogram reveals an ejection fraction of 33%. Which of the following best describes the respiratory pattern abnormality which occurs in this patient while sleeping?
A 60-year-old male presents with fatigue, dyspnea on exertion, and lower extremity edema. Physical examination reveals an elevated jugular venous pressure and an S3 heart sound. Which of the following medications is most likely to improve this patient's symptoms?
Practice by Chapter
Classification of heart failure (HFrEF vs HFpEF)
Practice Questions
Heart failure pathophysiology
Practice Questions
Acute decompensated heart failure
Practice Questions
Chronic heart failure management
Practice Questions
Guideline-directed medical therapy
Practice Questions
Device therapy for heart failure
Practice Questions
Cardiomyopathies
Practice Questions
Valvular heart disease and heart failure
Practice Questions
Right heart failure
Practice Questions
Pulmonary hypertension
Practice Questions
Cardio-renal syndrome
Practice Questions
Advanced heart failure and transplantation
Practice Questions
Quality measures in heart failure
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app