
Heart failure — MCQs

On this page
A 76-year-old woman seeks evaluation at a medical office for chest pain and shortness of breath on exertion of 3 months' duration. Physical examination shows bilateral pitting edema on the legs. On auscultation, diffuse crackles are heard over the lower lung fields. Cardiac examination shows jugular venous distention and an S3 gallop. Troponin is undetectable. A chest film shows cardiomegaly and pulmonary edema. Which of the following medications would be effective in lowering her risk of mortality?
A 31-year-old woman visits her primary care physician with the complaint that over the past 6 months she has "felt out of breath and dizzy while walking, even after short distances." She reports no other medical problems and denies taking any medications, vitamins, supplements, recreational drugs, alcohol or tobacco. Her BMI is 24kg/m2. On physical examination, the patient has a loud second heart sound over the left upper sternal border, increased jugular venous pressure, and a palpable right ventricular impulse. Which of the following is the patient most at risk of developing if her condition is allowed to persist for a prolonged period?
A 68-year-old man presents to your office concerned about the frequency with which he wakes up in the middle night feeling out of breath. He has been required to use 3 more pillows in order to reduce the shortness of breath. In addition to this, he has noticed that he tires easily with minor tasks such as walking 1 block, and more recently when he is dressing up in the mornings. Physical examination reveals a blood pressure of 120/85 mm Hg, heart rate of 82/min, respiratory rate of 20/min, and body temperature of 36.0°C (98.0°F). Cardiopulmonary examination reveals regular and rhythmic heart sounds with S4 gallop, a laterally displaced point of maximum impulse (PMI), and rales in both lung bases. He also presents with prominent hepatojugular reflux, orthopnea, and severe lower limb edema. Which of the following changes would be seen in this patient’s heart?
A 36-year-old man with a history of a stab wound to the right upper thigh one year previously presents to the emergency department with complaints of difficulty breathing while lying flat. Physical examination reveals an S3 gallop, hepatomegaly, warm skin and a continuous bruit over the right upper thigh. Which of the following is most likely responsible for his symptoms?
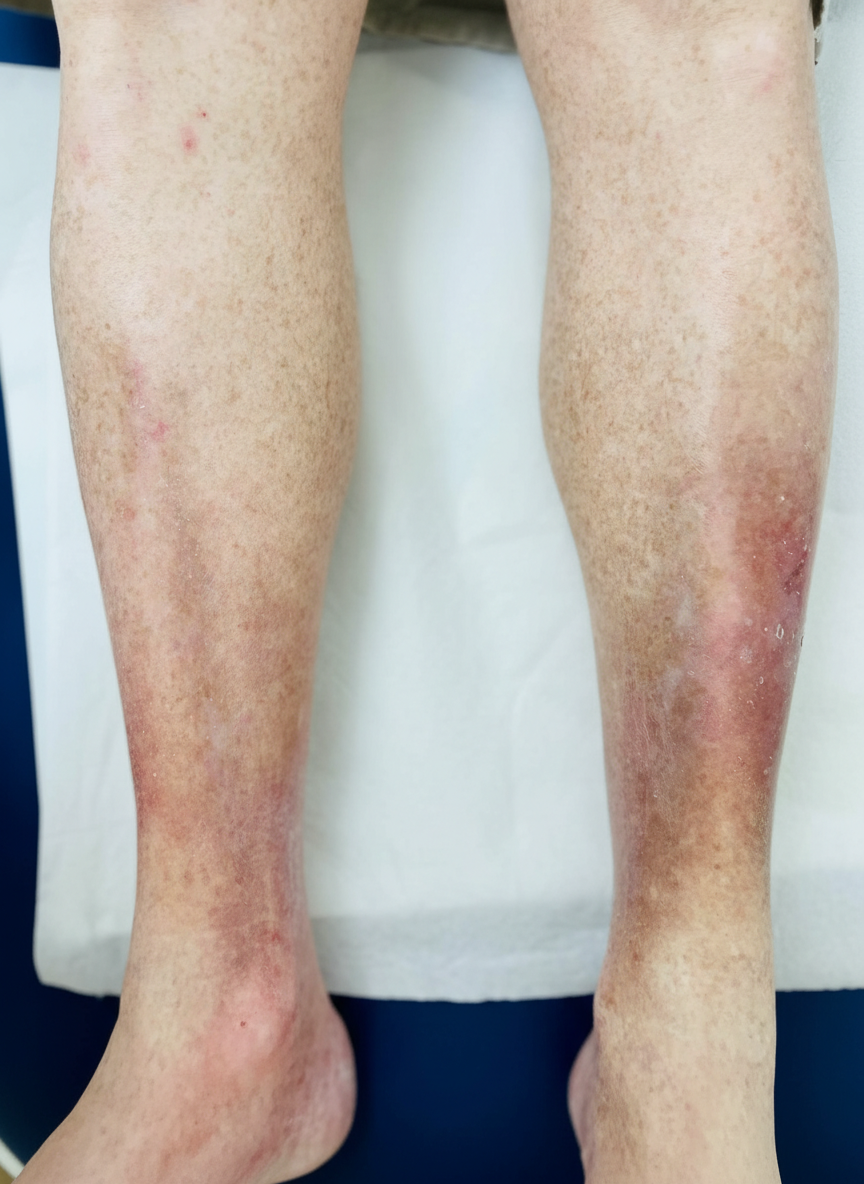
A 67-year-old woman comes to the physician with a 6-month history of pain and swelling of both legs. The symptoms are worst at the end of the day and are associated with itching of the overlying skin. Physical examination shows bilateral pitting ankle edema. An image of one of the ankles is shown. This patient is at greatest risk for which of the following complications?
A 28-year-old man presents to the clinic with increasing shortness of breath, mild chest pain at rest, and fatigue. He normally lives a healthy lifestyle with moderate exercise and an active social life, but recently he has been too tired to do much. He reports that he is generally healthy and on no medications but did have a ‘cold’ 2 weeks ago. He does not smoke, besides occasional marijuana with friends, and only drinks socially. His father has hypertension, hyperlipidemia, and lung cancer after a lifetime of smoking, and his mother is healthy. He also has one older brother with mild hypertension. His pulse is 104/min, the respiratory rate 23/min, the blood pressure 105/78 mm Hg, and the temperature 37.1°C (98.8°F). On physical examination, he is ill-appearing and has difficulty completing sentences. On auscultation he has a third heart sound, and his point of maximal impact is displaced laterally. He has 2+ pitting edema of the lower extremities up to the knees. An ECG is obtained and shows premature ventricular complexes and mildly widened QRS complexes. An echocardiogram is also performed and shows global hypokinesis with a left ventricle ejection fraction of 39%. Of the following, what is the most likely cause of his symptoms?
A 36-year-old man presents to his primary care physician because of shortness of breath. He is an office worker who has a mostly sedentary lifestyle; however, he has noticed that recently he feels tired and short of breath when going on long walks with his wife. He also has had a hacking cough that seems to linger, though he attributes this to an upper respiratory tract infection he had 2 months ago. He has diabetes that is well-controlled on metformin and has smoked 1 pack per day for 20 years. Physical exam reveals a large chested man with wheezing bilaterally and mild swelling in his legs and abdomen. The cause of this patient's abdominal and lower extremity swelling is most likely due to which of the following processes?
A 69-year-old man presents with progressive malaise, weakness, and confusion. The patient’s wife reports general deterioration over the last 3 days. He suffers from essential hypertension, but this is well controlled with amlodipine. He also has type 2 diabetes mellitus that is treated with metformin. On physical examination, the patient appears severely ill, weak and is unable to speak. His neck veins are distended bilaterally. His skin is mottled and dry with cool extremities, and he is mildly cyanotic. The respiratory rate is 24/min, the pulse is 94/min, the blood pressure is 87/64 mm Hg, and the temperature is 35.5°C (95.9°F). Auscultation yields coarse crackles throughout both lung bases. Which of the following best represents the mechanism of this patient’s condition?
A 66-year-old man presents to the emergency department with dyspnea. Two days ago, he hosted his grandchild's birthday party, and since has noticed general malaise, fever, and dry cough. He does not know if he feels more dyspneic while supine or standing but has noticed difficulty breathing even while watching television. He has a past medical history of congestive heart failure and hypertension, for which he takes aspirin, metoprolol, furosemide, lisinopril, and spironolactone as prescribed. His blood pressure is 90/50 mmHg, pulse is 120/min, and respirations are 30/min. His radial pulse is barely palpable, and his wrists and ankles are cold and clammy. Physical exam reveals a S3 and S4 with a soft holosystolic murmur at the apex, decreased breath sounds up to the middle lung fields, jugular venous distention to the auricles, and 3+ pitting edema to the mid thighs. EKG shows ST depressions consistent with demand ischemia. Bedside echocardiogram shows global akinesis with an ejection fraction (EF) of 20%; previous reports show EF at 40%. A portable chest radiograph shows bilateral pulmonary edema. Metoprolol is held, dobutamine and furosemide drips are started, and BiPAP is started at 20/5 cm H2O. After 15 minutes, the nurse reports that urine output is minimal and blood pressure is now 75/40 mmHg and pulse is 130/min. What is the best next step in management?
A 53-year-old white man presents to the emergency department because of progressive fatigue, shortness of breath on exertion, and a sensation of his heart pounding for the past 2 weeks. He has had high blood pressure for 8 years for which he takes hydrochlorothiazide. He denies any history of drug abuse or smoking, but he drinks alcohol socially. His blood pressure is 145/55 mm Hg, his radial pulse is 90/min and is bounding, and his temperature is 36.5°C (97.7°F). On physical examination, an early diastolic murmur is audible over the left sternal border. His chest X-ray shows cardiomegaly and echocardiography shows chronic, severe aortic regurgitation. If left untreated, which of the following is the most common long-term complication for this patient’s condition?
Practice by Chapter
Classification of heart failure (HFrEF vs HFpEF)
Practice Questions
Heart failure pathophysiology
Practice Questions
Acute decompensated heart failure
Practice Questions
Chronic heart failure management
Practice Questions
Guideline-directed medical therapy
Practice Questions
Device therapy for heart failure
Practice Questions
Cardiomyopathies
Practice Questions
Valvular heart disease and heart failure
Practice Questions
Right heart failure
Practice Questions
Pulmonary hypertension
Practice Questions
Cardio-renal syndrome
Practice Questions
Advanced heart failure and transplantation
Practice Questions
Quality measures in heart failure
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app