
Device therapy for heart failure — MCQs

A 71-year old man is brought to the emergency department because of progressively worsening shortness of breath and fatigue for 3 days. During the last month, he has also noticed dark colored urine. He had an upper respiratory infection 6 weeks ago. He underwent a cholecystectomy at the age of 30 years. He has hypertension, hyperlipidemia, and type 2 diabetes mellitus. He immigrated to the US from Italy 50 years ago. Current medications include simvastatin, lisinopril, and metformin. He appears pale. His temperature is 37.1°C (98.8°F), pulse is 96/min, respirations are 21/min, and blood pressure is 150/80 mm Hg. Auscultation of the heart shows a grade 4/6 systolic murmur over the right second intercostal space that radiates to the carotids. Laboratory studies show: Leukocyte count 9,000/mm3 Hemoglobin 8.3 g/dL Hematocrit 24% Platelet count 180,000/mm3 LDH 212 U/L Haptoglobin 15 mg/dL (N=41–165) Serum Na+ 138 mEq/L K+ 4.5 mEq/L CL- 102 mEq/L HCO3- 24 mEq/L Urea nitrogen 20 mg/dL Creatinine 1.2 mg/dL Total bilirubin 1.8 mg/dL Stool testing for occult blood is negative. Direct Coombs test is negative. Echocardiography shows an aortic jet velocity of 4.2 m/s and a mean pressure gradient of 46 mm Hg. Which of the following is the most appropriate next step in management to treat this patient's anemia?
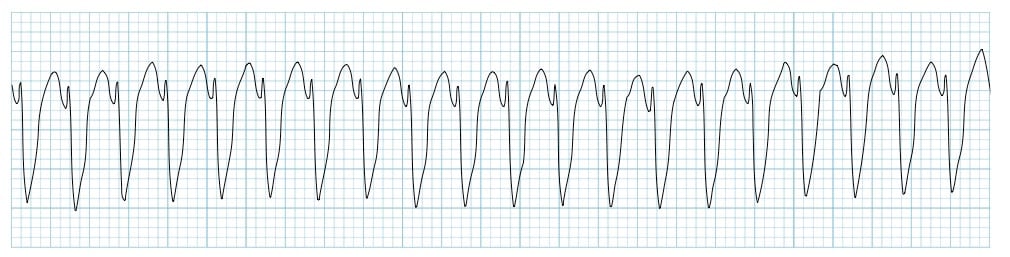
Two days after admission for myocardial infarction and subsequent coronary angioplasty, a 65-year-old man becomes distressed and diaphoretic in the cardiac intensive care unit. Suddenly he is no longer responsive. Pulse oximetry does not show a tracing. He has a history of hypertension and depression. Prior to his admission, his medication included ramipril and aripiprazole. Examination shows no carotid pulse. An ECG is shown. After beginning chest compressions, which of the following is the most appropriate step in management of the patient?
A 32-year-old woman comes to the physician because of worsening fatigue and shortness of breath. Her symptoms began 8 months ago and have progressively worsened since then. She had recurrent episodes of joint pain and fever during childhood. She does not smoke or drink alcohol. She emigrated from the Congo with her parents when she was 12 years old. Her temperature is 37.4°C (99.3°F), pulse is 90/min and regular, respirations are 18/min, and blood pressure is 140/90 mm Hg. There is an opening snap followed by a diastolic murmur at the fifth left intercostal space in the midclavicular line. If left untreated, this patient is at greatest risk for which of the following complications?
A 72-year-old man is taken to the emergency room after losing consciousness. According to his wife, he suddenly complained of fluttering in his chest, lightheadedness, and profuse sweating while walking to the grocery store. He then turned gray, lost consciousness, and collapsed onto the ground. His medical history is significant for a prior anterior wall myocardial infarction 2 years ago that was complicated by severe left ventricular systolic dysfunction. His blood pressure is 80/50 mm Hg, the temperature is 36.7°C (98.0°F), and the carotid pulse is not palpable. An ECG was obtained and the results are shown in the picture. Cardiopulmonary resuscitation is initiated and the patient is cardioverted to sinus rhythm with an external defibrillator. The patient regains consciousness and states there was no antecedent chest discomfort. Cardiac enzymes are negative and serum electrolytes are normal. Which of the following is the best next step for this patient?
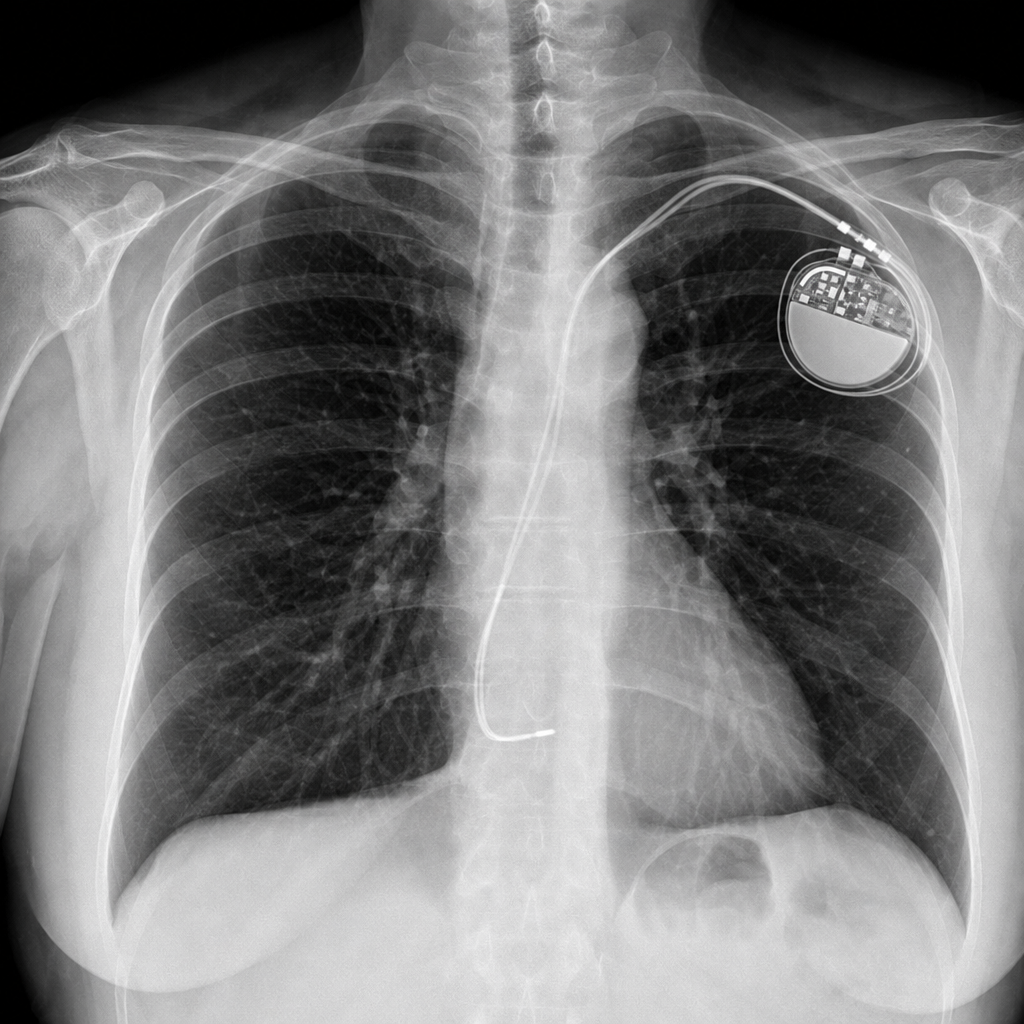
A 67-year-old woman comes to the emergency department because of a 4-month history of fatigue, shortness of breath with exertion, and dizziness. She has a history of atrial fibrillation and had a single-chamber pacemaker placed five years ago after an episode of syncope. Her pulse is 66/min and blood pressure is 98/66 mm Hg. An x-ray of the chest is shown. The x-ray confirms termination of the pacemaker lead in which of the following structures?
You are interested in studying the etiology of heart failure reduced ejection fraction (HFrEF) and attempt to construct an appropriate design study. Specifically, you wish to look for potential causality between dietary glucose consumption and HFrEF. Which of the following study designs would allow you to assess for and determine this causality?
A 71-year-old woman with a past medical history of type 2 diabetes, hypercholesterolemia, and hypertension was admitted to the hospital 8 hours ago with substernal chest pain for management of acute non-ST-elevated myocardial infarction (NSTEMI). The ECG findings noted by ST-depressions and T-wave inversions on anterolateral leads, which is also accompanied by elevated cardiac enzymes. Upon diagnosis, management with inhaled oxygen therapy, beta-blockers and aspirin, and low-molecular-weight heparin therapy were initiated, and she was placed on bed rest with continuous electrocardiographic monitoring. Since admission, she required 2 doses of sublingual nitroglycerin for recurrent angina, and the repeat troponin levels continued to rise. Given her risk factors, plans were made for early coronary angiography. The telemetry nurse calls the on-call physician because of her concern with the patient's mild confusion and increasing need for supplemental oxygen. At bedside evaluation, The vital signs include: heart rate 122/min, blood pressure 89/40 mm Hg, and the pulse oximetry is 91% on 6L of oxygen by nasal cannula. The telemetry and a repeat ECG show sinus tachycardia. She is breathing rapidly, appears confused, and complains of shortness of breath. On physical exam, the skin is cool and clammy and appears pale and dull. She has diffuse bilateral pulmonary crackles, and an S3 gallop is noted on chest auscultation with no new murmurs. She has jugular venous distention to the jaw-line, rapid and faint radial pulses, and 1+ dependent edema. She is immediately transferred to the intensive care unit for respiratory support and precautions for airway security. The bedside sonography shows abnormal hypodynamic anterior wall movement and an ejection fraction of 20%, but no evidence of mitral regurgitation or ventricular shunt. The chest X-ray demonstrates cephalization of pulmonary veins and pulmonary edema. What is the most appropriate next step in the stabilization of this patient?
A 62-year-old man with a past medical history of previous myocardial infarction, angina, hypertension, hyperlipidemia, diabetes mellitus, peripheral vascular disease, and below knee amputation has developed new chest pain. His medication includes insulin, hydrochlorothiazide, lisinopril, metoprolol, daily aspirin, atorvastatin, and nitroglycerin as needed. His vitals include: blood pressure 135/87 mm Hg, pulse 52/min, and respirations 17/min. Coronary arteriography shows a reduced ejection fraction, a 65% stenosis of the left anterior descending artery, and a 75% stenosis of the left circumflex artery. Which of the following is the recommended treatment for the patient?
A 58-year-old man is brought to the Emergency Department after 2 days of shortness of breath, orthopnea, and lower limb edema. His past medical history is significant for hypertension and a myocardial infarction 3 years ago that required a coronary arterial bypass graft. He has not been able to take prescribed medicine in several months due to recent unemployment and issues with insurance. On admission, his blood pressure is 155/92 mmHg, heart rate is 102/min, respiratory rate is 24/min, and temperature is 36.4°C (97.5°F). On physical examination there are fine rales in both lungs, regular and rhythmic cardiac sounds with an S3 gallop and a grade II/VI holosystolic murmur. Initial laboratory tests are shown below: Na+ 140 mEq/L K+ 4.2 mEq/L Cl- 105 mEq/L BUN 20 mg/dL Creatinine 0.8 mg/dL The patient is stabilized and admitted to the hospital. The next day his blood pressure is 110/60 mmHg, heart rate is 110/min, respiratory rate is 18/min, and temperature is 36.4°C (97.5°F). This morning's laboratory tests are shown below: Na+ 135 mEq/L K+ 3.2 mEq/L Cl- 102 mEq/L BUN 45 mg/dL Creatinine 1.7 mg/dL Which of the following best explains the changes seen in this patient?
A 55-year-old woman presents with fatigue, shortness of breath during ordinary activities, and occasional fluttering in her chest. She denies chest pain or lower extremity edema. She has no prior medical history. She does not smoke but drinks alcohol socially. Her blood pressure is 110/70 mm Hg, her temperature is 36.9°C (98.4°F), and her radial pulse is 95/min and regular. On physical examination, lungs are clear to auscultation, the apical impulse is slightly displaced, and a III/VI holosystolic murmur is audible at the apex and radiates to the axilla. Transthoracic echocardiography shows the presence of mitral regurgitation and an ejection fraction of 60 %. Which of the following is the optimal therapy for this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app