
Classification of heart failure (HFrEF vs HFpEF) — MCQs

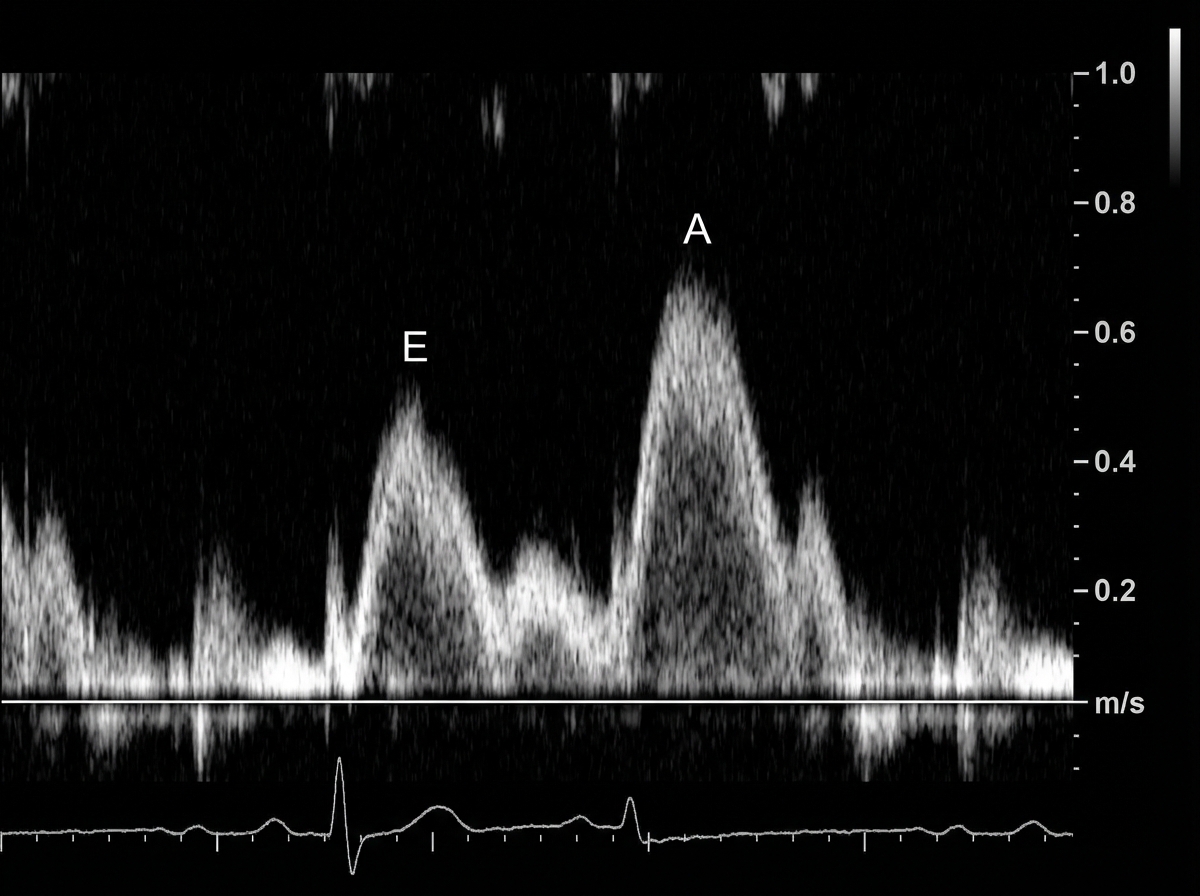
A 49-year-old man presents to his physician complaining of weakness and fatigue. On exam, you note significant peripheral edema. Transthoracic echocardiogram is performed and reveals a preserved ejection fraction with impaired diastolic relaxation. A representative still image is shown in Image A. Which of the following is likely the cause of this patient's symptoms?
A 76-year-old woman seeks evaluation at a medical office for chest pain and shortness of breath on exertion of 3 months' duration. Physical examination shows bilateral pitting edema on the legs. On auscultation, diffuse crackles are heard over the lower lung fields. Cardiac examination shows jugular venous distention and an S3 gallop. Troponin is undetectable. A chest film shows cardiomegaly and pulmonary edema. Which of the following medications would be effective in lowering her risk of mortality?
A 64-year-old man presents to his physician for a scheduled follow-up visit. He has chronic left-sided heart failure with systolic dysfunction. His current regular medications include captopril and digoxin, which were started after his last episode of symptomatic heart failure approximately 3 months ago. His last episode of heart failure was accompanied by atrial fibrillation, which followed an alcohol binge over a weekend. Since then he stopped drinking. He reports that he has no current symptoms at rest and is able to perform regular physical exercise without limitation. On physical examination, mild bipedal edema is noted. The physician suggested to him that he should discontinue digoxin and continue captopril and scheduled him for the next follow-up visit. Which of the following statements best justifies the suggestion made by the physician?
The serum brain natriuretic peptide and N-terminal pro-BNP are elevated. A diagnosis of heart failure with preserved ejection fraction is made. In addition to supplemental oxygen therapy, which of the following is the most appropriate initial step in management?
On cardiology service rounds, your team sees a patient admitted with an acute congestive heart failure exacerbation. In congestive heart failure, decreased cardiac function leads to decreased renal perfusion, which eventually leads to excess volume retention. To test your knowledge of physiology, your attending asks you which segment of the nephron is responsible for the majority of water absorption. Which of the following is a correct pairing of the segment of the nephron that reabsorbs the majority of all filtered water with the means by which that segment absorbs water?
A 60-year-old male engineer who complains of shortness of breath when walking a few blocks undergoes a cardiac stress test because of concern for coronary artery disease. During the test he asks his cardiologist about what variables are usually used to quantify the functioning of the heart. He learns that one of these variables is stroke volume. Which of the following scenarios would be most likely to lead to a decrease in stroke volume?
A 64-year-old male with a history of coronary artery disease, hypertension, hyperlipidemia, and type II diabetes presents to his primary care physician with increasing shortness of breath and ankle swelling over the past month. Which of the following findings is more likely to be seen in left-sided heart failure and less likely to be seen in right-sided heart failure?
A 71-year-old woman with a past medical history of type 2 diabetes, hypercholesterolemia, and hypertension was admitted to the hospital 8 hours ago with substernal chest pain for management of acute non-ST-elevated myocardial infarction (NSTEMI). The ECG findings noted by ST-depressions and T-wave inversions on anterolateral leads, which is also accompanied by elevated cardiac enzymes. Upon diagnosis, management with inhaled oxygen therapy, beta-blockers and aspirin, and low-molecular-weight heparin therapy were initiated, and she was placed on bed rest with continuous electrocardiographic monitoring. Since admission, she required 2 doses of sublingual nitroglycerin for recurrent angina, and the repeat troponin levels continued to rise. Given her risk factors, plans were made for early coronary angiography. The telemetry nurse calls the on-call physician because of her concern with the patient's mild confusion and increasing need for supplemental oxygen. At bedside evaluation, The vital signs include: heart rate 122/min, blood pressure 89/40 mm Hg, and the pulse oximetry is 91% on 6L of oxygen by nasal cannula. The telemetry and a repeat ECG show sinus tachycardia. She is breathing rapidly, appears confused, and complains of shortness of breath. On physical exam, the skin is cool and clammy and appears pale and dull. She has diffuse bilateral pulmonary crackles, and an S3 gallop is noted on chest auscultation with no new murmurs. She has jugular venous distention to the jaw-line, rapid and faint radial pulses, and 1+ dependent edema. She is immediately transferred to the intensive care unit for respiratory support and precautions for airway security. The bedside sonography shows abnormal hypodynamic anterior wall movement and an ejection fraction of 20%, but no evidence of mitral regurgitation or ventricular shunt. The chest X-ray demonstrates cephalization of pulmonary veins and pulmonary edema. What is the most appropriate next step in the stabilization of this patient?
A 72-year-old woman comes to the emergency department because of a 2-week history of worsening shortness of breath, lower extremity swelling, and a 3-kg (6.6-lb) weight gain. Crackles are heard on auscultation of the chest. Cardiac examination shows a dull, low-pitched early diastolic sound at the 5th left intercostal space that becomes louder in the left lateral decubitus position at end-expiration. Which of the following is the most likely cause of these auscultation findings?
Background: Beta-blockers reduce mortality in patients who have chronic heart failure, systolic dysfunction, and are on background treatment with diuretics and angiotensin-converting enzyme inhibitors. We aimed to compare the effects of carvedilol and metoprolol on clinical outcome. Methods: In a multicenter, double-blind, randomized parallel group trial, we assigned 1511 patients with chronic heart failure to treatment with carvedilol (target dose, 25 mg twice daily) and 1518 to metoprolol (target dose, 50 mg twice daily). The patients were required to have chronic heart failure (NYHA II-IV), the previous admission for a cardiovascular indication, an ejection fraction of < 0.35, and to have been treated optimally with diuretics and angiotensin-converting enzyme inhibitors unless not tolerated. The primary endpoints were all-cause mortality and the composite endpoint of all-cause mortality or all-cause admission. The analysis was done by intention-to-treat. Findings: The mean study duration was 58 months (SD, 6). The mean ejection fraction was 0.26 (SD, 0.07) and the mean age was 62 years (SD, 11). The all-cause mortality was 34% (512 of 1511) for carvedilol and 40% (600 of 1518) for metoprolol (hazard ratio, 0.83 [95% CI 0.74-0.93], p = 0.0017). The reduction in all-cause mortality was consistent across pre-defined subgroups. The incidence of side effects and drug withdrawals did not differ significantly between the 2 study groups. Based on the best interpretation of the results of this clinical trial, which of the following statements is most accurate?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app