
Chronic heart failure management — MCQs

The serum brain natriuretic peptide and N-terminal pro-BNP are elevated. A diagnosis of heart failure with preserved ejection fraction is made. In addition to supplemental oxygen therapy, which of the following is the most appropriate initial step in management?
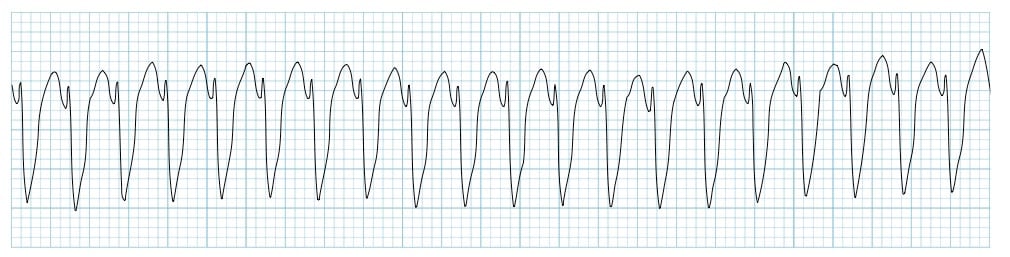
A 72-year-old man is taken to the emergency room after losing consciousness. According to his wife, he suddenly complained of fluttering in his chest, lightheadedness, and profuse sweating while walking to the grocery store. He then turned gray, lost consciousness, and collapsed onto the ground. His medical history is significant for a prior anterior wall myocardial infarction 2 years ago that was complicated by severe left ventricular systolic dysfunction. His blood pressure is 80/50 mm Hg, the temperature is 36.7°C (98.0°F), and the carotid pulse is not palpable. An ECG was obtained and the results are shown in the picture. Cardiopulmonary resuscitation is initiated and the patient is cardioverted to sinus rhythm with an external defibrillator. The patient regains consciousness and states there was no antecedent chest discomfort. Cardiac enzymes are negative and serum electrolytes are normal. Which of the following is the best next step for this patient?
A 70-year-old Caucasian male visits your office regularly for treatment of New York Heart association class IV congestive heart failure. Which of the following medications would you add to this man's drug regimen in order to improve his overall survival?
A 59-year-old man presents to his primary care provider with the complaint of daytime fatigue. He often has a headache that is worse in the morning and feels tired when he awakes. He perpetually feels fatigued even when he sleeps in. The patient lives alone, drinks 2-3 beers daily, drinks coffee regularly, and has a 10 pack-year smoking history. His temperature is 99.0°F (37.2°C), blood pressure is 180/110 mm Hg, pulse is 80/min, respirations are 13/min, and oxygen saturation is 98% on room air. Physical exam is notable for a BMI of 39 kg/m^2. The rest of the patient's pulmonary and neurological exams are unremarkable. Which of the following is the best next step in management?
A 56-year-old woman comes to the physician for follow-up after a measurement of elevated blood pressure at her last visit three months ago. She works as a high school teacher at a local school. She says that she mostly eats cafeteria food and take-out. She denies any regular physical activity. She does not smoke or use any recreational drugs. She drinks 2 to 3 glasses of wine per day. She has hypercholesterolemia for which she takes atorvastatin. Her height is 165 cm (5 ft 5 in), weight is 82 kg (181 lb), and BMI is 30.1 kg/m2. Her pulse is 67/min, respirations are 18/min, and blood pressure is 152/87 mm Hg on the right arm and 155/92 mm Hg on the left arm. She would like to try lifestyle modifications to improve her blood pressure before considering pharmacologic therapy. Which of the following lifestyle modifications is most likely to result in the greatest reduction of this patient's systolic blood pressure?
A 36-year-old man presents to his primary care physician because of shortness of breath. He is an office worker who has a mostly sedentary lifestyle; however, he has noticed that recently he feels tired and short of breath when going on long walks with his wife. He also has had a hacking cough that seems to linger, though he attributes this to an upper respiratory tract infection he had 2 months ago. He has diabetes that is well-controlled on metformin and has smoked 1 pack per day for 20 years. Physical exam reveals a large chested man with wheezing bilaterally and mild swelling in his legs and abdomen. The cause of this patient's abdominal and lower extremity swelling is most likely due to which of the following processes?
A 70-year-old male presents for an annual exam. His past medical history is notable for shortness of breath when he sleeps, and upon exertion. Recently he has experienced dyspnea and lower extremity edema that seems to be worsening. Both of these symptoms have resolved since he was started on several medications and instructed to weigh himself daily. Which of the following is most likely a component of his medical management?
A 36-year-old man with a history of a stab wound to the right upper thigh one year previously presents to the emergency department with complaints of difficulty breathing while lying flat. Physical examination reveals an S3 gallop, hepatomegaly, warm skin and a continuous bruit over the right upper thigh. Which of the following is most likely responsible for his symptoms?
A 59-year-old woman presents to the physician for a 3-month history of progressively worsening shortness of breath on exertion and swelling of her legs. She has a history of breast cancer that was treated with surgery, followed by doxorubicin and cyclophosphamide therapy 4 years ago. Cardiac examination shows an S3 gallop, but there are no murmurs or rubs. Examination of the lower extremities shows pitting edema below the knees. Echocardiography is most likely to show which of the following sets of changes in this patient? Aorto-ventricular pressure gradient Diastolic function Ventricular cavity size Ventricular wall thickness A Normal ↓ Normal Normal B Normal Normal ↑ ↑ C Normal ↓ ↑ ↑ D ↑ ↓ ↑ ↑ E Normal Normal ↑ ↓
A 66-year-old man presents to the emergency department with dyspnea. Two days ago, he hosted his grandchild's birthday party, and since has noticed general malaise, fever, and dry cough. He does not know if he feels more dyspneic while supine or standing but has noticed difficulty breathing even while watching television. He has a past medical history of congestive heart failure and hypertension, for which he takes aspirin, metoprolol, furosemide, lisinopril, and spironolactone as prescribed. His blood pressure is 90/50 mmHg, pulse is 120/min, and respirations are 30/min. His radial pulse is barely palpable, and his wrists and ankles are cold and clammy. Physical exam reveals a S3 and S4 with a soft holosystolic murmur at the apex, decreased breath sounds up to the middle lung fields, jugular venous distention to the auricles, and 3+ pitting edema to the mid thighs. EKG shows ST depressions consistent with demand ischemia. Bedside echocardiogram shows global akinesis with an ejection fraction (EF) of 20%; previous reports show EF at 40%. A portable chest radiograph shows bilateral pulmonary edema. Metoprolol is held, dobutamine and furosemide drips are started, and BiPAP is started at 20/5 cm H2O. After 15 minutes, the nurse reports that urine output is minimal and blood pressure is now 75/40 mmHg and pulse is 130/min. What is the best next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app