
Advanced heart failure and transplantation — MCQs

A 10-year-old boy is presented to the hospital for a kidney transplant. In the operating room, the surgeon connects an allograft kidney renal artery to the aorta, and after a few moments, the kidney becomes cyanotic, edematous, and dusky with mottling. Which of the following in the recipient’s serum is responsible for this rejection?
A 56-year-old man comes to the emergency department because of progressively worsening shortness of breath and fever for 2 days. He also has a nonproductive cough. He does not have chest pain or headache. He has chronic myeloid leukemia and had a bone marrow transplant 3 months ago. His current medications include busulfan, mycophenolate mofetil, tacrolimus, and methylprednisolone. His temperature is 38.1°C (100.6°F), pulse is 103/min, respirations are 26/min, and blood pressure is 130/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 93%. Pulmonary examination shows diffuse crackles. The spleen tip is palpated 4 cm below the left costal margin. Laboratory studies show: Hemoglobin 10.3 g/dL Leukocyte count 4,400/mm3 Platelet count 160,000/mm3 Serum Glucose 78 mg/dL Creatinine 2.1 mg/dL D-dimer 96 ng/mL (N < 250) pp65 antigen positive Galactomannan antigen negative Urinalysis is normal. An x-ray of the chest shows diffuse bilateral interstitial infiltrates. An ECG shows sinus tachycardia. Which of the following is the most appropriate pharmacotherapy?
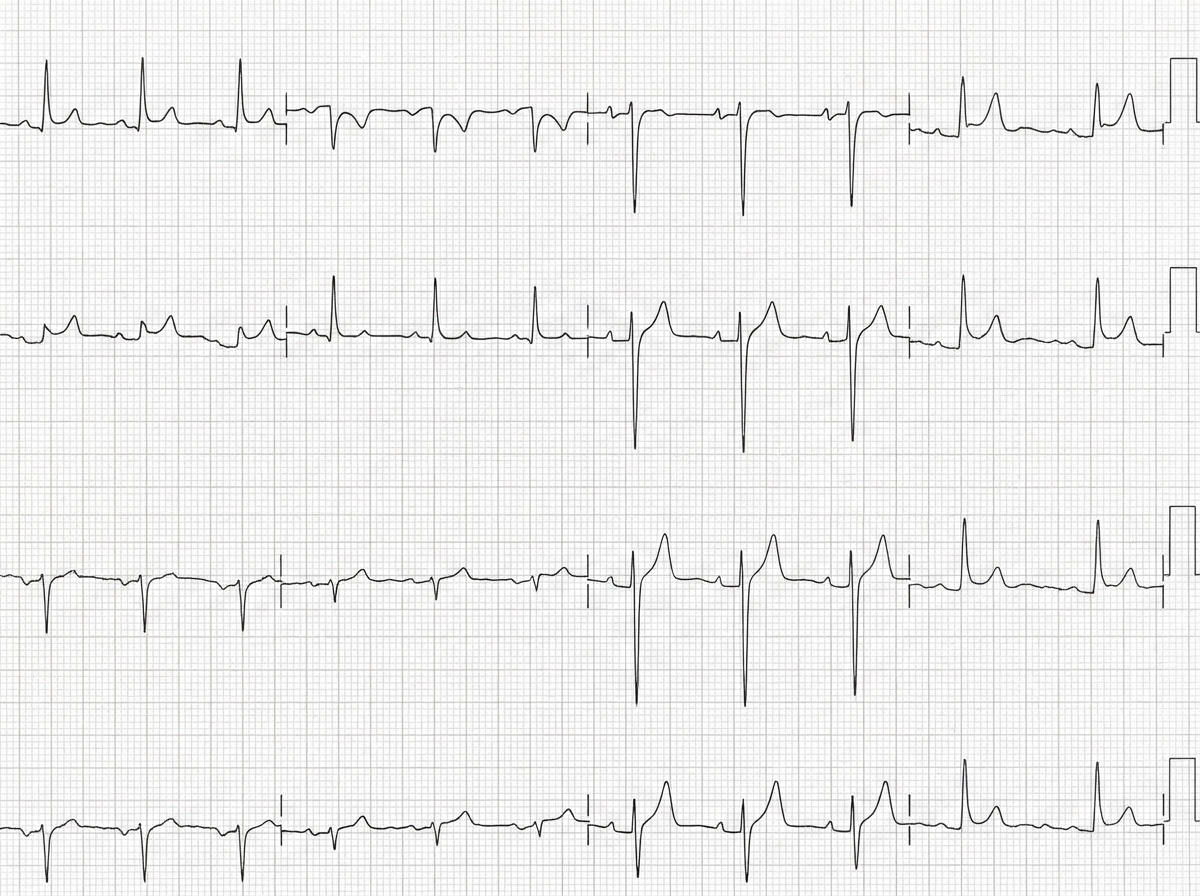
A 50-year-old man with a history of stage 4 kidney disease was admitted to the hospital for an elective hemicolectomy. His past medical history is significant for severe diverticulitis. After the procedure he becomes septic and was placed on broad spectrum antibiotics. On morning rounds, he appear weak and complains of fatigue and nausea. His words are soft and he has difficulty answering questions. His temperature is 38.9°C (102.1°F), heart rate is 110/min, respiratory rate is 15/min, blood pressure 90/65 mm Hg, and saturation is 89% on room air. On physical exam, his mental status appears altered. He has a bruise on his left arm that spontaneously appeared overnight. His cardiac exam is positive for a weak friction rub. Blood specimens are collected and sent for evaluation. An ECG is performed (see image). What therapy will this patient most likely receive next?
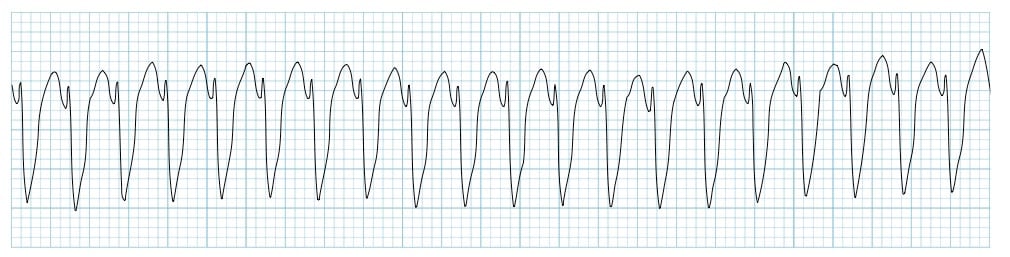
A 72-year-old man is taken to the emergency room after losing consciousness. According to his wife, he suddenly complained of fluttering in his chest, lightheadedness, and profuse sweating while walking to the grocery store. He then turned gray, lost consciousness, and collapsed onto the ground. His medical history is significant for a prior anterior wall myocardial infarction 2 years ago that was complicated by severe left ventricular systolic dysfunction. His blood pressure is 80/50 mm Hg, the temperature is 36.7°C (98.0°F), and the carotid pulse is not palpable. An ECG was obtained and the results are shown in the picture. Cardiopulmonary resuscitation is initiated and the patient is cardioverted to sinus rhythm with an external defibrillator. The patient regains consciousness and states there was no antecedent chest discomfort. Cardiac enzymes are negative and serum electrolytes are normal. Which of the following is the best next step for this patient?
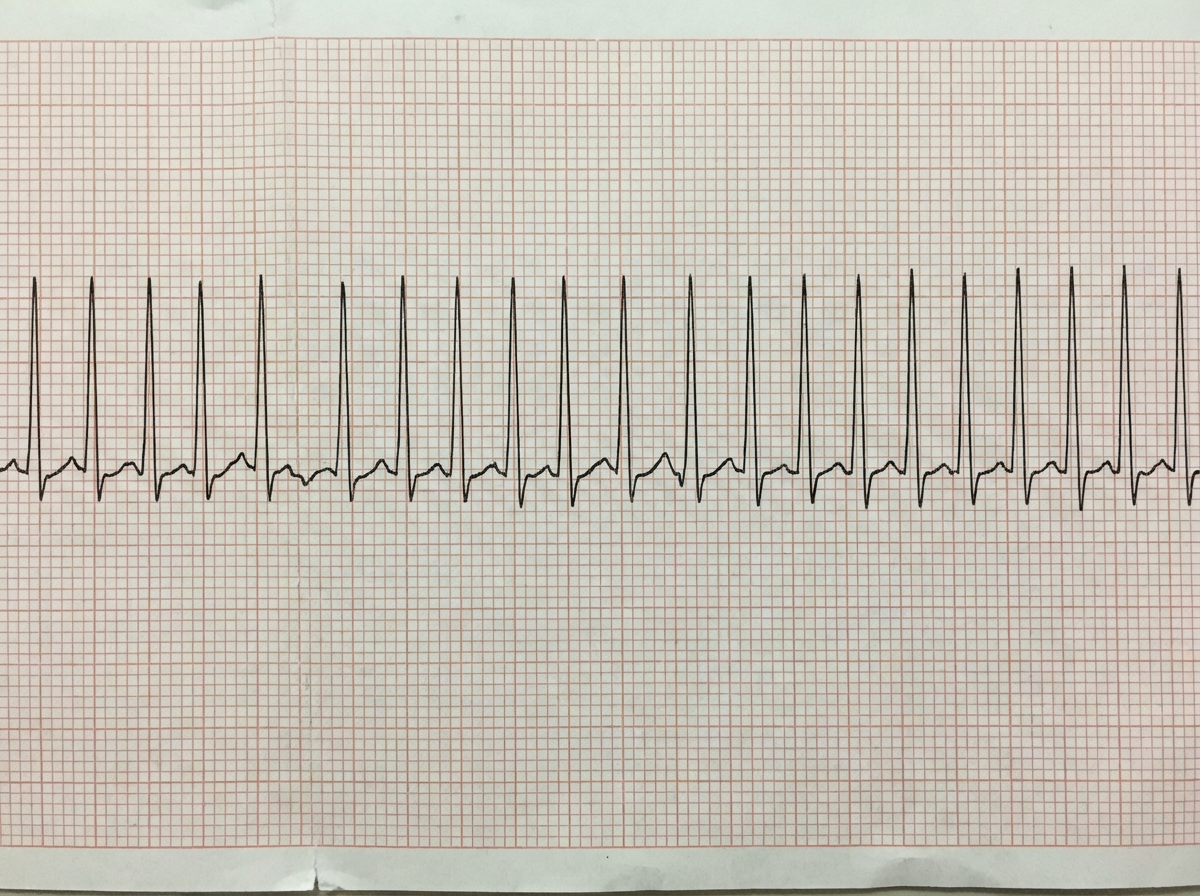
A previously healthy 33-year-old woman comes to the emergency department because she could feel her heart racing intermittently for the last 2 hours. Each episode lasts about 10 minutes. She does not have any chest pain. Her mother died of a heart attack and her father had an angioplasty 3 years ago. She has smoked a half pack of cigarettes daily for 14 years. She drinks one to two beers daily. She appears anxious. Her temperature is 37.6°C (98.1°F), pulse is 160/min, and blood pressure is 104/76 mm Hg. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. An ECG is shown. Which of the following is the most appropriate initial step in management?
A 43-year-old woman presents to the emergency department complaining of palpitations, dry cough, and shortness of breath for 1 week. She immigrated to the United States from Korea at the age of 20. She says that her heart is racing and she has never felt these symptoms before. Her cough is dry and is associated with shortness of breath that occurs with minimal exertion. Her past medical history is otherwise unremarkable. She has no allergies and is not currently taking any medications. She is a nonsmoker and an occasional drinker. She denies illicit drug use. Her blood pressure is 100/65 mm Hg, pulse is 76/min, respiratory rate is 23/min, and temperature is 36.8°C (98.2°F). Her physical examination is significant for bibasilar lung crackles and a non-radiating, low-pitched, mid-diastolic rumbling murmur best heard at the apical region. In addition, she has jugular vein distention and bilateral pitting edema in her lower extremities. Which of the following best describes the infectious agent that led to this patient’s condition?
A 72-year-old woman is brought to the emergency department by ambulance after an unexpected fall at home 1 hour ago. She was resuscitated at the scene by paramedics before being transferred to the hospital. She has a history of ischemic heart disease and type 2 diabetes mellitus. She has not taken any sedative medications. Her GCS is 6. She is connected to a mechanical ventilator. Her medical records show that she signed a living will 5 years ago, which indicates her refusal to receive any type of cardiopulmonary resuscitation, intubation, or maintenance of life support on mechanical ventilation. Her son, who has a durable power-of-attorney for her healthcare decisions, objects to the discontinuation of mechanical ventilation and wishes that his mother be kept alive without suffering in the chance that she might recover. Which of the following is the most appropriate response to her son regarding his wishes for his mother?
A 71-year-old woman with a past medical history of type 2 diabetes, hypercholesterolemia, and hypertension was admitted to the hospital 8 hours ago with substernal chest pain for management of acute non-ST-elevated myocardial infarction (NSTEMI). The ECG findings noted by ST-depressions and T-wave inversions on anterolateral leads, which is also accompanied by elevated cardiac enzymes. Upon diagnosis, management with inhaled oxygen therapy, beta-blockers and aspirin, and low-molecular-weight heparin therapy were initiated, and she was placed on bed rest with continuous electrocardiographic monitoring. Since admission, she required 2 doses of sublingual nitroglycerin for recurrent angina, and the repeat troponin levels continued to rise. Given her risk factors, plans were made for early coronary angiography. The telemetry nurse calls the on-call physician because of her concern with the patient's mild confusion and increasing need for supplemental oxygen. At bedside evaluation, The vital signs include: heart rate 122/min, blood pressure 89/40 mm Hg, and the pulse oximetry is 91% on 6L of oxygen by nasal cannula. The telemetry and a repeat ECG show sinus tachycardia. She is breathing rapidly, appears confused, and complains of shortness of breath. On physical exam, the skin is cool and clammy and appears pale and dull. She has diffuse bilateral pulmonary crackles, and an S3 gallop is noted on chest auscultation with no new murmurs. She has jugular venous distention to the jaw-line, rapid and faint radial pulses, and 1+ dependent edema. She is immediately transferred to the intensive care unit for respiratory support and precautions for airway security. The bedside sonography shows abnormal hypodynamic anterior wall movement and an ejection fraction of 20%, but no evidence of mitral regurgitation or ventricular shunt. The chest X-ray demonstrates cephalization of pulmonary veins and pulmonary edema. What is the most appropriate next step in the stabilization of this patient?
A 72-year-old woman comes to the emergency department because of a 2-week history of worsening shortness of breath, lower extremity swelling, and a 3-kg (6.6-lb) weight gain. Crackles are heard on auscultation of the chest. Cardiac examination shows a dull, low-pitched early diastolic sound at the 5th left intercostal space that becomes louder in the left lateral decubitus position at end-expiration. Which of the following is the most likely cause of these auscultation findings?
The serum brain natriuretic peptide and N-terminal pro-BNP are elevated. A diagnosis of heart failure with preserved ejection fraction is made. In addition to supplemental oxygen therapy, which of the following is the most appropriate initial step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app