
Acute decompensated heart failure — MCQs

An investigator is studying patients with acute decompensated congestive heart failure. He takes measurements of a hormone released from atrial myocytes, as well as serial measurements of left atrial and left ventricular pressures. The investigator observes a positive correlation between left atrial pressures and the serum level of this hormone. Which of the following is most likely the mechanism of action of this hormone?
The serum brain natriuretic peptide and N-terminal pro-BNP are elevated. A diagnosis of heart failure with preserved ejection fraction is made. In addition to supplemental oxygen therapy, which of the following is the most appropriate initial step in management?
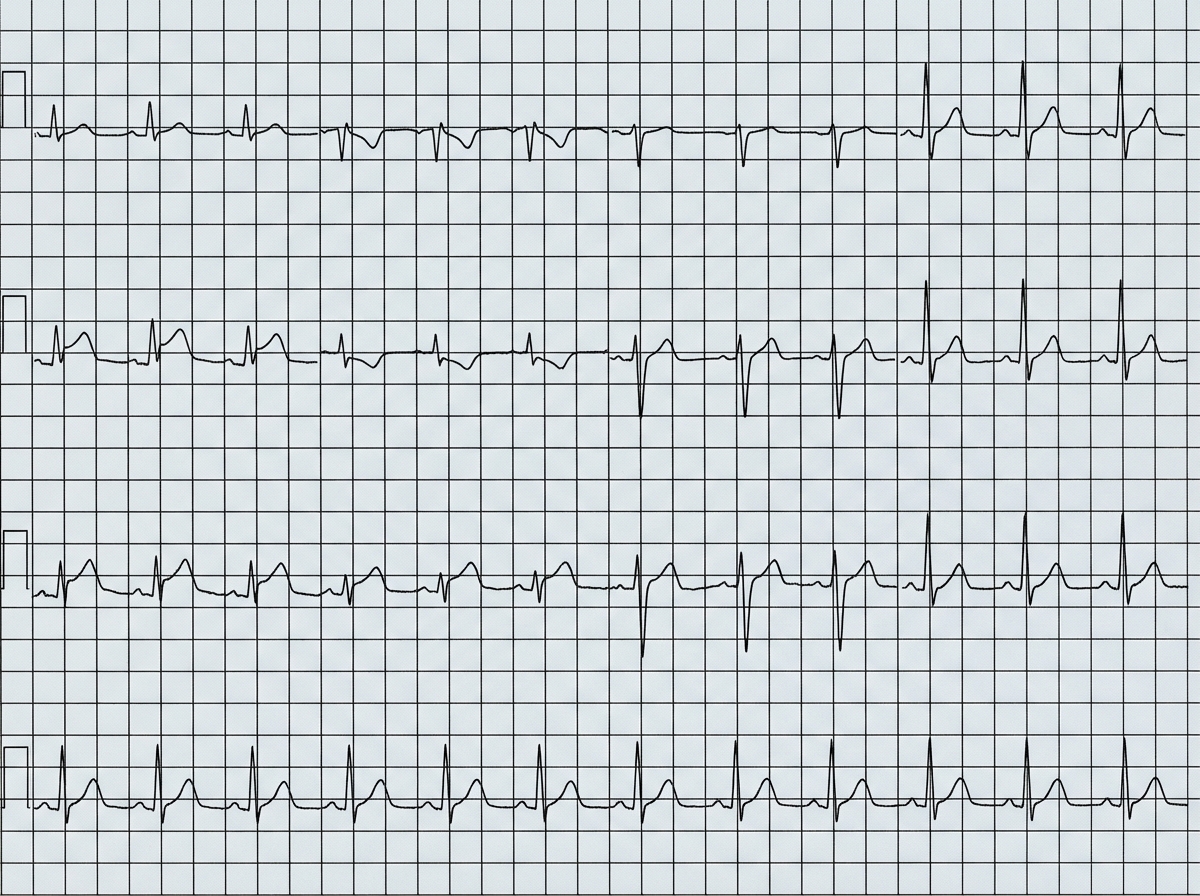
A 54-year-old man is brought to the emergency department 1 hour after the sudden onset of shortness of breath, epigastric pain, and sweating. He has no history of similar symptoms. He has hypertension and type 2 diabetes mellitus. Current medications include amlodipine and metformin. He has smoked one pack of cigarettes daily for 20 years. He appears weak and pale. His pulse is 56/min, respirations are 18/min, and blood pressure is 100/70 mm Hg. Cardiac examination shows normal heart sounds. The lungs are clear to auscultation. The skin is cold to the touch. An ECG is shown. Bedside transthoracic echocardiography shows normal left ventricular function. High-dose aspirin is administered. Administration of which of the following is most appropriate next step in management?
An 81-year-old man is admitted to the hospital due to acute decompensated heart failure. He has type 2 diabetes mellitus, hypertension, coronary artery disease, and congestive heart failure. Current medications include lisinopril, metformin, and low-dose aspirin. He has smoked one pack of cigarettes daily for 45 years. His temperature is 37.6°C (99.7°F), pulse is 105/min and regular, respirations are 21/min, and blood pressure is 103/64 mm Hg. Laboratory studies show: Hemoglobin 13.7 g/dL Leukocyte count 8200/mm3 Serum Na+ 128 mEq/L Cl- 98 mEq/L K+ 4.9 mEq/L Urea nitrogen 58 mg/dL Glucose 200 mg/dL Creatinine 2.2 mg/dL Which of the following changes in the medication regimen is most appropriate in this patient at this time?
A 70-year-old Caucasian male visits your office regularly for treatment of New York Heart association class IV congestive heart failure. Which of the following medications would you add to this man's drug regimen in order to improve his overall survival?
A 62-year-old man is brought to the emergency department because of progressive shortness of breath, mild chest pain on exertion, and a cough for 2 days. One week ago, he had a low-grade fever and nasal congestion. He has hypertension but does not adhere to his medication regimen. He has smoked one pack of cigarettes daily for 30 years and drinks 3–4 beers daily. His temperature is 37.1°C (98.8°F), pulse is 125/min, respirations are 29/min, and blood pressure is 145/86 mm Hg. He is in moderate respiratory distress while sitting. Pulmonary examination shows reduced breath sounds bilaterally. There is scattered wheezing over all lung fields. There is inward displacement of his abdomen during inspiration. Arterial blood gas analysis shows: pH 7.29 PCO2 63 mm Hg PO2 71 mm Hg HCO3- 29 mEq/L O2 saturation 89% Which of the following is the most likely cause of this patient's symptoms?
A 59-year-old woman comes to the physician for a 3-month history of progressively worsening shortness of breath on exertion and swelling of her legs. She has a history of breast cancer, which was treated with surgery followed by therapy with doxorubicin and trastuzumab 4 years ago. Cardiac examination shows an S3 gallop; there are no murmurs or rubs. Examination of the lower extremities shows pitting edema below the knees. Echocardiography is most likely to show which of the following sets of changes in this patient? $$$ Ventricular wall thickness %%% Ventricular cavity size %%% Diastolic function %%% Aorto-ventricular pressure gradient $$$
A 66-year-old man presents to the emergency department with dyspnea. Two days ago, he hosted his grandchild's birthday party, and since has noticed general malaise, fever, and dry cough. He does not know if he feels more dyspneic while supine or standing but has noticed difficulty breathing even while watching television. He has a past medical history of congestive heart failure and hypertension, for which he takes aspirin, metoprolol, furosemide, lisinopril, and spironolactone as prescribed. His blood pressure is 90/50 mmHg, pulse is 120/min, and respirations are 30/min. His radial pulse is barely palpable, and his wrists and ankles are cold and clammy. Physical exam reveals a S3 and S4 with a soft holosystolic murmur at the apex, decreased breath sounds up to the middle lung fields, jugular venous distention to the auricles, and 3+ pitting edema to the mid thighs. EKG shows ST depressions consistent with demand ischemia. Bedside echocardiogram shows global akinesis with an ejection fraction (EF) of 20%; previous reports show EF at 40%. A portable chest radiograph shows bilateral pulmonary edema. Metoprolol is held, dobutamine and furosemide drips are started, and BiPAP is started at 20/5 cm H2O. After 15 minutes, the nurse reports that urine output is minimal and blood pressure is now 75/40 mmHg and pulse is 130/min. What is the best next step in management?
A 71-year-old woman with a past medical history of type 2 diabetes, hypercholesterolemia, and hypertension was admitted to the hospital 8 hours ago with substernal chest pain for management of acute non-ST-elevated myocardial infarction (NSTEMI). The ECG findings noted by ST-depressions and T-wave inversions on anterolateral leads, which is also accompanied by elevated cardiac enzymes. Upon diagnosis, management with inhaled oxygen therapy, beta-blockers and aspirin, and low-molecular-weight heparin therapy were initiated, and she was placed on bed rest with continuous electrocardiographic monitoring. Since admission, she required 2 doses of sublingual nitroglycerin for recurrent angina, and the repeat troponin levels continued to rise. Given her risk factors, plans were made for early coronary angiography. The telemetry nurse calls the on-call physician because of her concern with the patient's mild confusion and increasing need for supplemental oxygen. At bedside evaluation, The vital signs include: heart rate 122/min, blood pressure 89/40 mm Hg, and the pulse oximetry is 91% on 6L of oxygen by nasal cannula. The telemetry and a repeat ECG show sinus tachycardia. She is breathing rapidly, appears confused, and complains of shortness of breath. On physical exam, the skin is cool and clammy and appears pale and dull. She has diffuse bilateral pulmonary crackles, and an S3 gallop is noted on chest auscultation with no new murmurs. She has jugular venous distention to the jaw-line, rapid and faint radial pulses, and 1+ dependent edema. She is immediately transferred to the intensive care unit for respiratory support and precautions for airway security. The bedside sonography shows abnormal hypodynamic anterior wall movement and an ejection fraction of 20%, but no evidence of mitral regurgitation or ventricular shunt. The chest X-ray demonstrates cephalization of pulmonary veins and pulmonary edema. What is the most appropriate next step in the stabilization of this patient?
A 36-year-old man presents to his primary care physician because of shortness of breath. He is an office worker who has a mostly sedentary lifestyle; however, he has noticed that recently he feels tired and short of breath when going on long walks with his wife. He also has had a hacking cough that seems to linger, though he attributes this to an upper respiratory tract infection he had 2 months ago. He has diabetes that is well-controlled on metformin and has smoked 1 pack per day for 20 years. Physical exam reveals a large chested man with wheezing bilaterally and mild swelling in his legs and abdomen. The cause of this patient's abdominal and lower extremity swelling is most likely due to which of the following processes?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app