
Heart failure — MCQs

On this page
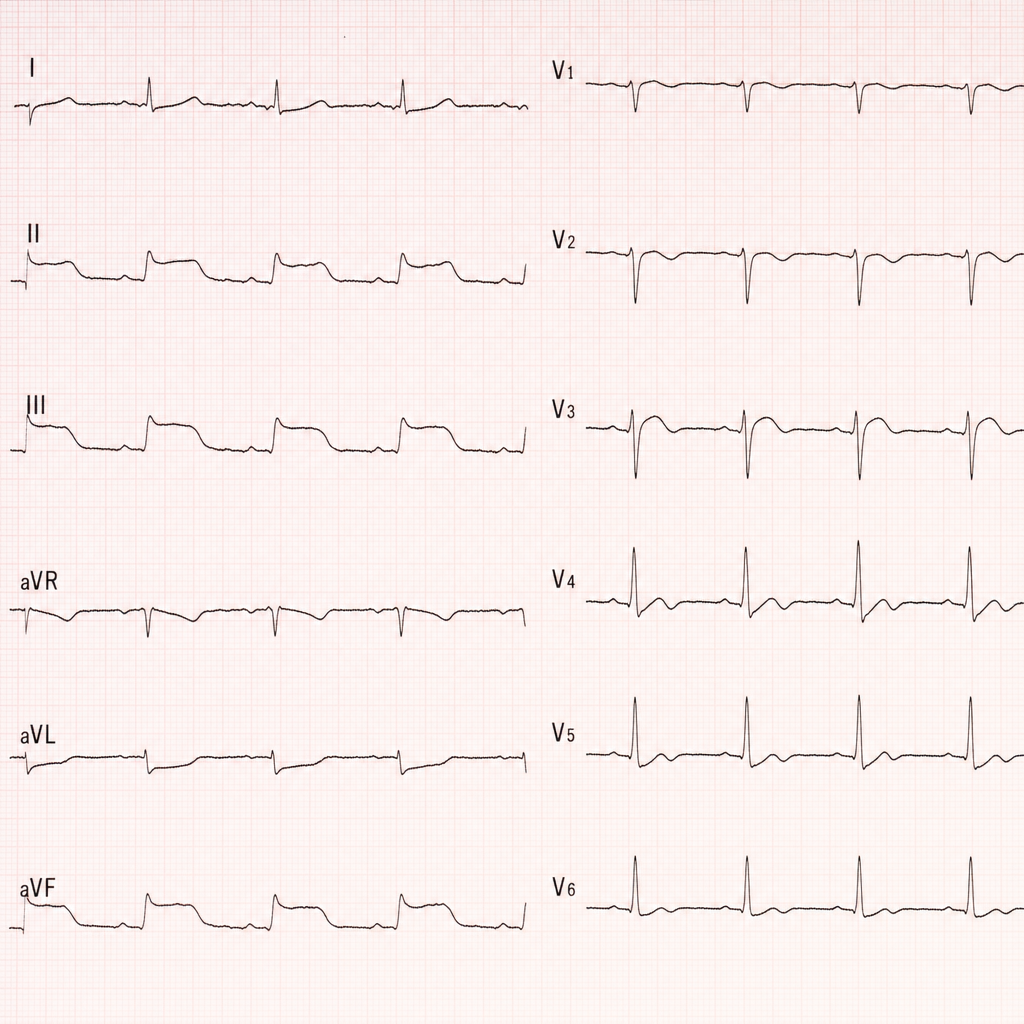
A 68-year-old man with a history of hypertension and type 2 diabetes presents to the emergency department with 2 hours of crushing substernal chest pain radiating to his left arm, diaphoresis, and nausea. BP is 88/60 mmHg, HR is 112 bpm, RR is 22/min, and SpO₂ is 94% on room air. The ECG shows ST elevations in leads II, III, and aVF with reciprocal ST depressions in leads I and aVL, consistent with an acute inferior STEMI. Crackles are heard at both lung bases. The nearest cardiac catheterization laboratory is 3 hours away by transport. Which of the following is the most appropriate immediate reperfusion strategy?
A 55-year-old woman comes to the emergency department because of epigastric pain, sweating, and breathlessness for 45 minutes. She has hypertension treated with hydrochlorothiazide. She has smoked 1 pack of cigarettes daily for the past 30 years and drinks 1 glass of wine daily. Her pulse is 105/min and blood pressure is 100/70 mm Hg. Arterial blood gas analysis on room air shows: pH 7.49 pCO2 32 mm Hg pO2 57 mm Hg Which of the following is the most likely cause of hypoxemia in this patient?
A 34-year-old woman, gravida 2, para 2, is admitted to the hospital because of shortness of breath and fatigue 2 weeks after delivery of a full-term female newborn. She has no history of major medical illness. Cardiac examination on admission shows an S3 gallop and a grade 2/6 holosystolic murmur heard best at the apex. Treatment is initiated with intravenous furosemide and captopril. Her symptoms resolve, and 3 weeks later, cardiac examination shows no murmur. Which of the following is the most likely explanation for the initial auscultation findings?
A 25-year-old man comes to the emergency department because of a 1-week-history of progressively worsening dyspnea and intermittent chest pain that increases on inspiration. He had an upper respiratory tract infection 2 weeks ago. His pulse is 115/min and blood pressure is 100/65 mm Hg. Examination shows inspiratory crackles bilaterally. His serum troponin I is 0.21 ng/mL (N < 0.1). An x-ray of the chest shows an enlarged cardiac silhouette and prominent vascular markings in both lung fields; costophrenic angles are blunted. A rhythm strip shows inverted T waves. Which of the following additional findings is most likely in this patient's condition?
A 65-year-old man comes to the physician for a follow-up examination. He has chronic obstructive pulmonary disease and was recently discharged from the hospital for an exacerbation. His cough and chills have since improved, but his mobility is still severely limited by dyspnea and fatigue. He smoked 2 packs of cigarettes daily for 30 years, but quit 5 years ago. His medications include inhaled daily budesonide, formoterol, and tiotropium bromide plus ipratropium/albuterol as needed. Pulmonary function testing shows an FEV1 of 27% of predicted. Resting oxygen saturation ranges from 84–88%. Which of the following steps in management is most likely to increase the chance of survival in this patient?
Practice by Chapter
Classification of heart failure (HFrEF vs HFpEF)
Practice Questions
Heart failure pathophysiology
Practice Questions
Acute decompensated heart failure
Practice Questions
Chronic heart failure management
Practice Questions
Guideline-directed medical therapy
Practice Questions
Device therapy for heart failure
Practice Questions
Cardiomyopathies
Practice Questions
Valvular heart disease and heart failure
Practice Questions
Right heart failure
Practice Questions
Pulmonary hypertension
Practice Questions
Cardio-renal syndrome
Practice Questions
Advanced heart failure and transplantation
Practice Questions
Quality measures in heart failure
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app