
Gastroenterology — MCQs

On this page
A 61-year-old man with HIV comes to the physician because of a 3-week history of fatigue, nonproductive cough, and worsening shortness of breath. He appears ill. Pulse oximetry on room air shows an oxygen saturation of 89%. Laboratory studies show a CD4+ T-lymphocyte count of 67/mm3 (N ≥ 500/mm3) and an elevated HIV viral load. An x-ray of the chest shows diffuse interstitial infiltrates bilaterally. A bronchoalveolar lavage shows disc-shaped yeast cells. In addition to starting antiretroviral therapy, the appropriate treatment for the patient's current illness is initiated. Maintaining the patient on a medication to prevent recurrence of his current illness will also prevent which of the following conditions?
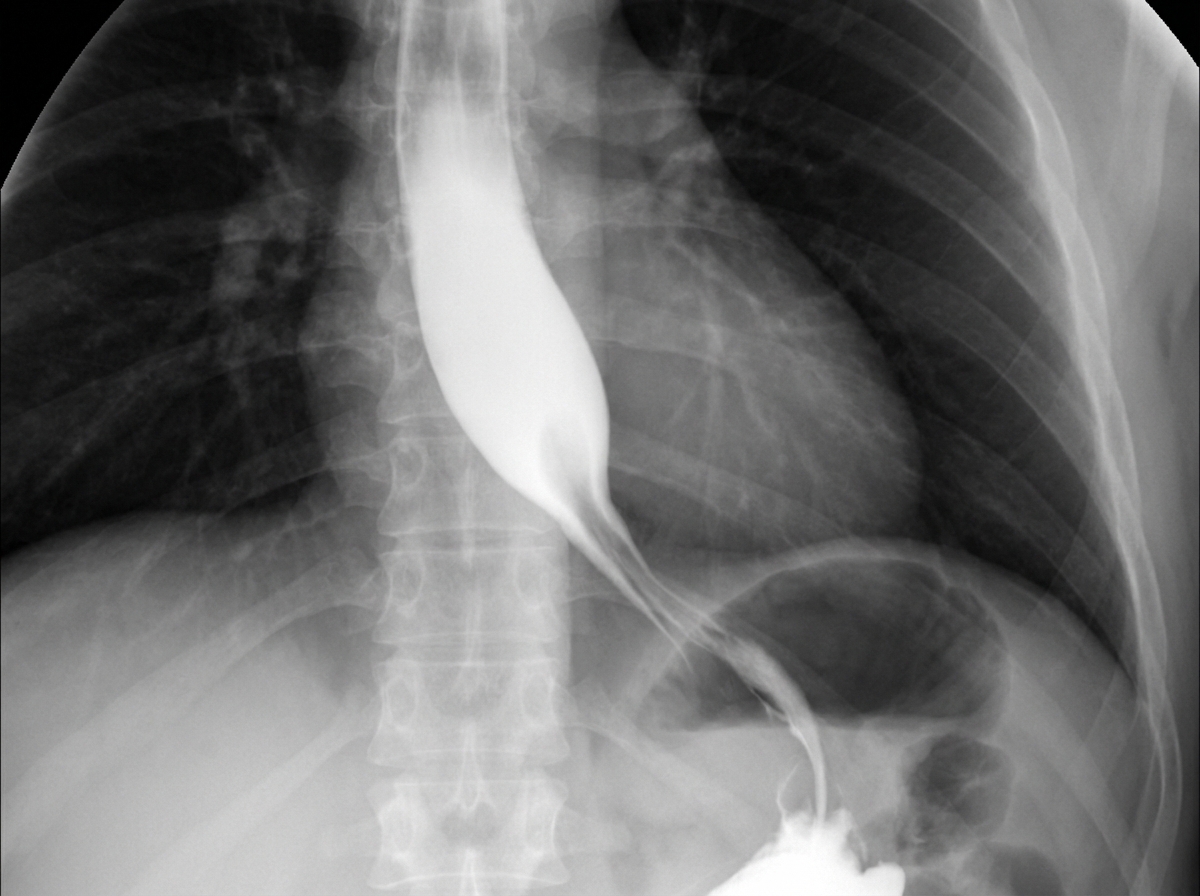
A 56-year-old woman comes to the physician because of a 6-month history of difficulty swallowing food. Initially, only solid food was problematic, but liquids have also become more difficult to swallow over the last 2 months. She also reports occasional regurgitation of food when she lies down. The patient is an avid birdwatcher and returned from a 3-week trip to the Amazon rainforest 3 months ago. She has had a 3.5-kg (7.7-lb) weight loss over the past 6 months. She has not had abdominal pain, blood in her stools, or fever. She underwent an abdominal hysterectomy for fibroid uterus 6 years ago. She has smoked a pack of cigarettes daily for 25 years. Current medications include metformin and sitagliptin. The examination shows no abnormalities. Her hemoglobin concentration is 12.2 g/dL. A barium esophagram is shown. Esophageal manometry monitoring shows the lower esophageal sphincter fails to relax during swallowing. Which of the following is the next best step in management?
A 57-year-old woman presents to her primary care physician with complaints of nausea, vomiting, abdominal pain, and bloating that have increased in severity over the past several months. She reports that she occasionally vomits after eating. She states that the emesis contains undigested food particles. Additionally, the patient states that she often is satiated after only a few bites of food at meals. Her medical history is significant for hypertension and type II diabetes mellitus. Initial laboratory values are notable only for a hemoglobin A1c of 14%. Which of the following is the best initial treatment for this patient?
A 63-year-old man comes to the physician because of a 2-day history of redness, swelling, and pain of the right leg. He also has fever, chills, and nausea. He has noticed liquid oozing from the affected area on his right leg. He has a history of hypertension and gastroesophageal reflux disease. Three months ago, he was hospitalized for treatment of a hip fracture. His current medications include metoprolol, enalapril, and omeprazole. His temperature is 38.7°C (101.7°F), pulse is 106/min, and blood pressure is 142/94 mm Hg. Examination of the right lower leg shows a large area of erythema with poorly-demarcated borders and purulent drainage. The area is nonfluctuant, warm, and tender to touch. Examination of the right groin shows several enlarged, tender lymph nodes. There is mild edema of the ankles bilaterally. Blood and wound cultures are collected. Which of the following is the best next step in management?
A 47-year-old woman presents with weakness, shortness of breath, and lightheadedness. She says her symptoms onset gradually 4 months ago and have progressively worsened. Past medical history is significant for a long history of menorrhagia secondary to uterine fibroids. Her vital signs include: temperature 36.9°C (98.4°F), blood pressure 135/82 mm Hg, and pulse 97/min. Physical examination is unremarkable. Laboratory test results are shown below: Hemoglobin 9.2 g/dL Mean corpuscular volume (MCV) 74 μm3 Mean corpuscular hemoglobin (MCH) 21 pg/cell Reticulocyte count 0.4 % Serum ferritin 10 ng/mL Which of the following is a specific feature of this patient's condition?
A 32-year-old male patient presents to a medical office requesting screening for colorectal cancer. He currently has no symptoms and his main concern is that his father was diagnosed with colorectal cancer at 55 years of age. What screening strategy would be the most appropriate?
A 55-year-old female presents to clinic with recurrent episodes of abdominal discomfort and pain for the past month. She reports that the pain occurs 2-3 hours after meals, usually at midnight, and rates it as moderate to severe in intensity when it occurs. She also complains of being fatigued all the time. Past medical history is insignificant. She is an office secretary and says that the job has been very stressful recently. Her temperature is 98.6°F (37.0°C), respiratory rate is 15/min, pulse is 67/min, and blood pressure is 122/98 mm Hg. Her BMI is 34. A physical examination reveals conjunctival pallor and mild tenderness over her epigastric region. Blood tests show: Hb%: 10 gm/dL Total count (WBC): 11,000 /mm3 Differential count: Neutrophils: 70% Lymphocytes: 25% Monocytes: 5% ESR: 10 mm/hr Which of the following is the most likely diagnosis?
A 72-year-old man presents to his primary care physician with the symptom of generalized malaise over the last month. He also has abdominal pain that has been persistent and not relieved by ibuprofen. He has unintentionally lost 22 pounds recently. During this time, the patient has experienced intermittent diarrhea when he eats large meals. The patient has a past medical history of alcohol use, obesity, diabetes mellitus, hypertension, IV drug use, and asthma. His current medications include disulfiram, metformin, insulin, atorvastatin, lisinopril, albuterol, and an inhaled corticosteroid. The patient attends weekly Alcoholics Anonymous meetings and was recently given his two week chip for not drinking. His temperature is 99.5°F (37.5°C), blood pressure is 100/57 mmHg, pulse is 88/min, respirations are 11/min, and oxygen saturation is 98% on room air. The patient's abdomen is tender to palpation, and the liver edge is palpable 2 cm inferior to the rib cage. Neurologic exam demonstrates gait that is not steady. Which of the following is the best initial diagnostic test for this patient?
A 44-year-old woman comes to the emergency department because of a 10-hour history of severe nausea and abdominal pain that began 30 minutes after eating dinner. The pain primarily is in her right upper quadrant and occasionally radiates to her back. She has a history of type 2 diabetes mellitus and hypercholesterolemia. Current medications include metformin and atorvastatin. She is 163 cm (5 ft 4 in) tall and weighs 91 kg (200 lb); BMI is 34 kg/m2. Her temperature is 38.8°C (101.8°F), pulse is 100/min, respirations are 14/min, and blood pressure is 150/76 mm Hg. Abdominal examination shows right upper quadrant tenderness with guarding. A bedside ultrasound shows a gall bladder wall measuring 6 mm, pericholecystic fluid, sloughing of the intraluminal membrane, and a 2 x 2-cm stone at the neck of the gallbladder. The common bile duct appears unremarkable. Laboratory studies show leukocytosis and normal liver function tests. Intravenous fluids are started, and she is given ketorolac for pain control. Which of the following is the most appropriate next step in management?
A 45-year-old man presents to the office for evaluation of pruritic skin lesions, which he has had for 1 month on his elbows and knees. He has been using over-the-counter ointments, but they have not helped. He has not seen a healthcare provider for many years. He has no known allergies. His blood pressure is 140/80 mm Hg, his pulse is 82 beats per minute, his respirations are 18 breaths per minute, and his temperature is 37.2°C (98.9°F). On examination, clustered vesicular lesions are noted on both elbows and knees. Cardiovascular and pulmonary exams are unremarkable. Which of the following would most likely be associated with this patient’s condition?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app