
Gastroenterology — MCQs

On this page
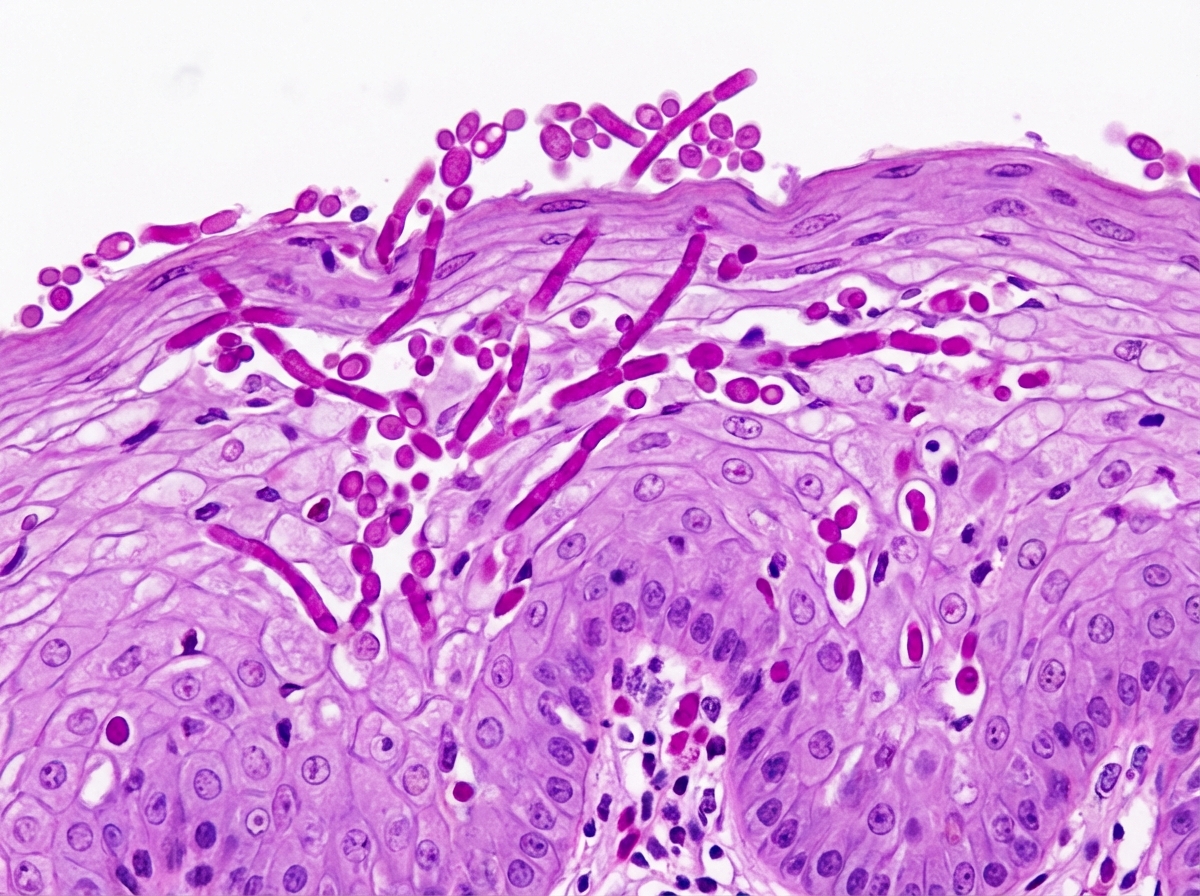
A 44-year-old man presents to a clinic for the evaluation of difficulty swallowing for the past few days. He says that he has noticed progressively worsening chest pain when he attempts to swallow solids or liquids. He works from a home office, has not had any recent sick contacts, and is currently not sexually active. His medical history includes AIDS. His current medications include emtricitabine, rilpivirine, and tenofovir. His temperature is 38.1°C (100.6°F), pulse is 72/min, respirations are 18/min, and blood pressure is 136/84 mm Hg. A physical examination is notable for a dry mouth with red mucosa and no distinct plaques or patches, and a supple neck with no masses or cervical lymphadenopathy. An esophagogastroduodenoscopy shows small white patches within the esophageal lumen. A biopsy of one of the lesions is performed and the microscopic appearance of the finding is shown below. Which of the following is the most likely diagnosis?
A 36-year-old Caucasian woman is referred to the outpatient clinic by a physician at a health camp for 6-months of foul-smelling diarrhea with bulky and floating stools as well as significant flatulence which makes her extremely uncomfortable at work and social events. She has concomitant weight loss and recently fractured her wrist in a seemingly insignificant fall from her own height. Vital signs are normal and a physical examination shows grouped, papulovesicular, pruritic skin lesions, as well as areas of hypoesthesia in the hands and feet. Which of the following would be most useful in this case?
A 73-year-old man presents to his primary care physician complaining of increased urinary frequency, nocturia, and incomplete emptying after void. He is otherwise healthy, with no active medical problems. On examination, a large, symmetric, firm, smooth prostate is palpated, but otherwise the exam is normal. Which of the following is a potential complication of the patient's present condition?
A 52-year-old woman with HIV infection is brought to the emergency department 20 minutes after she had a generalized tonic-clonic seizure. She appears lethargic and confused. Laboratory studies show a CD4+ count of 89 cells/μL (N > 500). A CT scan of the head with contrast shows multiple ring-enhancing lesions in the basal ganglia and subcortical white matter. An India ink preparation of cerebrospinal fluid is negative. Which of the following is the most likely diagnosis?
A 52-year-old woman presents to her primary care provider with colicky left flank pain that radiates to her groin. She appears to be in significant distress and is having trouble getting comfortable on the exam table. She and her mother both have a history of calcium oxalate kidney stones. She has a past medical history significant for type 2 diabetes and hypertension. She takes metformin, metoprolol and lisinopril. She has been watching her weight and eating a high protein diet that mainly consists of chicken and seafood. She also eats a great deal of yogurt for the calcium. She asks if she should cut out the yogurt, and wonders if it is the cause of her current kidney stone. What lifestyle modification would reduce her risk of developing kidney stones in the future?
A 45-year-old woman comes to the physician because of a 4-month history of irritability and frequent bowel movements. During this time, she has had a 6.8-kg (15-lb) weight loss. She has not had a change in appetite or diet. She takes no medications. Her temperature is 37.4°C (99.4°F), pulse is 112/min, respirations are 16/min, and blood pressure is 126/74 mm Hg. Examination shows moist palms. The thyroid gland is diffusely enlarged; there are no palpable nodules. Serum studies show a thyroid-stimulating hormone (TSH) concentration of 0.2 μU/mL, thyroxine (T4) concentration of 22 μg/dL, and antibodies against the TSH receptor. Which of the following treatment modalities is associated with the lowest rate of recurrence for this patient's condition?
Four days after undergoing a Whipple procedure for newly-diagnosed pancreatic cancer, a 65-year-old man has shortness of breath. His surgery was complicated by bleeding for which he required intraoperative transfusion with 4 units of packed red blood cells and 1 unit of platelets. His temperature is 38.8°C (101.8°F), pulse is 110/min, respirations are 26/min, and blood pressure is 95/55 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 85%. Cardiac examination shows normal heart sounds and no jugular venous distention. Auscultation of the lungs shows diffuse crackles bilaterally. The extremities are warm and there is no edema. Laboratory studies show a leukocyte count of 17,000/mm3 and hemoglobin concentration of 9.8 g/dL. Arterial blood gas on room air shows: pH 7.35 PaO2 41 mm Hg PaCO2 38 mm Hg HCO3- 25 mEq/L The patient is intubated and mechanical ventilation is initiated. An x-ray of the chest is shown. Transthoracic echocardiography shows a normally contracting left ventricle. Which of the following is the most likely cause of this patient's current condition?

A 44-year-old woman comes to the physician because of a 3-week history of progressive pain while swallowing. She has the feeling that food gets stuck in her throat and is harder to swallow than usual. She has a history of high-grade cervical dysplasia which was treated with conization 12 years ago. Four months ago, she was diagnosed with Graves' disease and started on antithyroid therapy. Her last menstrual period was 3 weeks ago. She has had 8 lifetime sexual partners and uses condoms inconsistently. Her father died of stomach cancer. She has never smoked and drinks one glass of wine daily. She uses cocaine occasionally. Her current medications include methimazole and a vitamin supplement. Her temperature is 37°C (98.6°F), pulse is 75/min, respirations are 18/min, and blood pressure is 110/75 mm Hg. Examination of the oral cavity shows several white plaques that can be scraped off easily. The lungs are clear to auscultation. Laboratory studies show: Hemoglobin 11.9 g/dL Leukocyte count 12,200/mm3 Platelet count 290,000/mm3 Prothrombin time 12 seconds Partial thromboplastin time (activated) 38 seconds Serum pH 7.33 Na+ 135 mEq/L Cl- 104 mEq/L K+ 4.9 mEq/L HCO3- 24 mEq/L Blood urea nitrogen 13 mg/dL Glucose 110 mg/dL Creatinine 1.1 mg/dL HIV test positive In addition to starting antiretroviral therapy, which of the following is the most appropriate next step in management?
A 24-year-old man presents to the emergency department with sudden onset of fever for the past few hours as well as pain and swelling in his right knee and left ankle. He denies any recent history of trauma or injury. The patient is otherwise a healthy, active young man. He recently recovered from a case of gastroenteritis which caused significant abdominal pain and bloody stool 4 weeks ago. He believes the infection was related to eating undercooked chicken while camping. His blood pressure is 124/76 mm Hg, his heart rate is 76/min, and his temperature is 36.9 ℃ (98.4 ℉). Physical examination reveals tenderness to palpation of his right knee and left ankle as well as erythematous conjunctiva. Which of the following features would be least likely to develop in patients with this condition?
A 55-year-old woman with type 2 diabetes mellitus comes to the physician for evaluation of worsening tingling of her feet at night for the last 6 months. Two years ago, she underwent retinal laser photocoagulation in both eyes. She admits to not adhering to her insulin regimen. Her blood pressure is 130/85 mm Hg while sitting and 118/70 mm Hg while standing. Examination shows decreased sense of vibration and proprioception in her toes and ankles bilaterally. Her serum hemoglobin A1C is 11%. Urine dipstick shows 2+ protein. Which of the following additional findings is most likely in this patient?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app