
Gastroenterology — MCQs

On this page
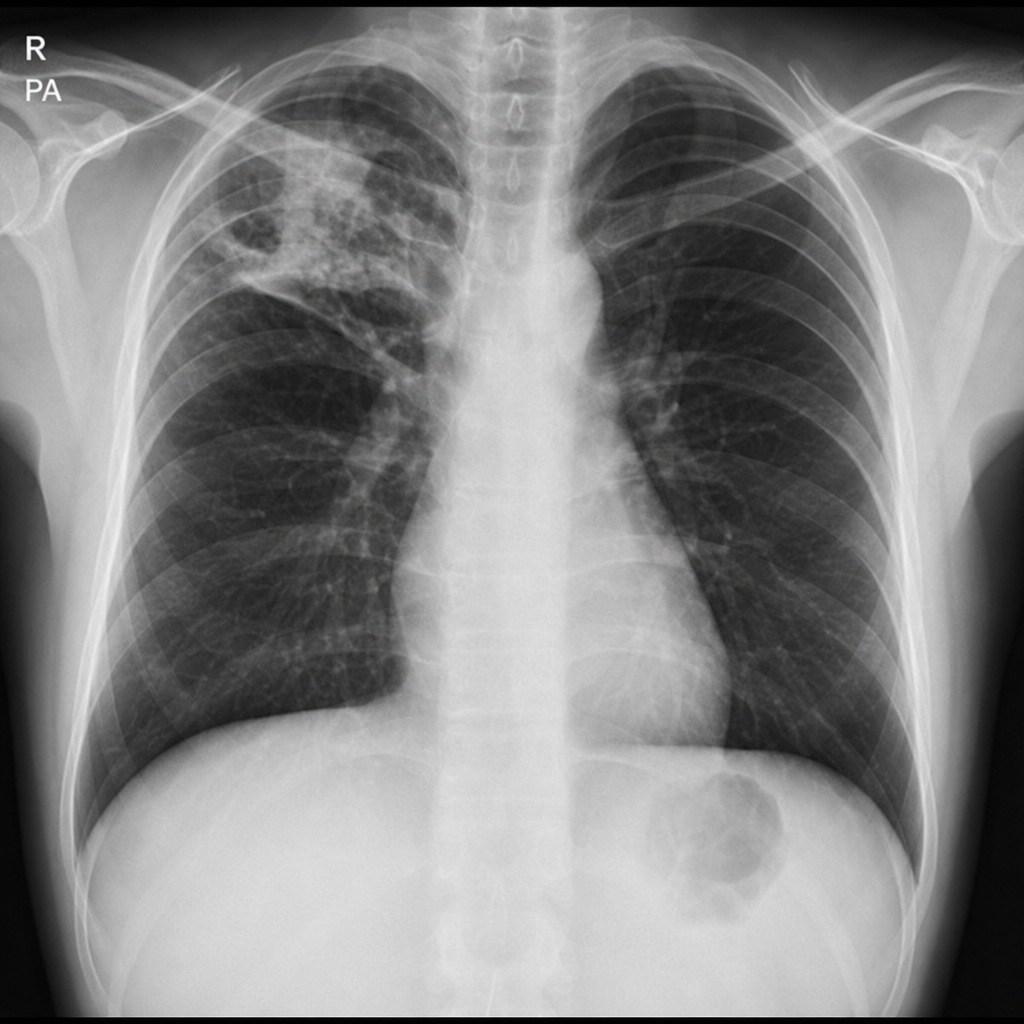
A 35-year-old man who recently emigrated from a country with a high prevalence of tuberculosis presents with 3 weeks of cough, night sweats, and weight loss. Chest radiography shows a right upper-lobe cavitary opacity with surrounding infiltrate, as shown. Which of the following is the most appropriate initial management?
A 42-year-old woman presents complaining of pain in her hands. She reports that the pain is in both hands, and that it is usually worse in the morning. She reports that her hands are also stiff in the morning, but that this gradually improves throughout the morning. She notes, however, that her symptoms seem to be getting worse over the last three months. What is the most likely pathogenesis of her disease process?
A 24-year-old African American college student comes to the office for a scheduled visit. He has been healthy, although he reports occasional flank discomfort which comes and goes. He denies any fever, chills, dysuria, or polyuria in the past year. His vaccinations are up to date. His family history is unknown, as he was adopted. He smokes 1 pack of cigarettes every 3 days, drinks socially, and denies any current illicit drug use, although he endorses a history of injection drug use. He currently works as a waiter to afford his college tuition. His physical examination shows a young man with a lean build, normal heart sounds, clear breath sounds, bowel sounds within normal limits, and no lower extremity edema. You order a urinalysis which shows 8 red blood cells (RBCs) per high-power field (HPF). The test is repeated several weeks later and shows 6 RBCs/HPF. What is the most appropriate next step in management?
A 24-year-old man comes to the physician for the evaluation of a severely pruritic skin rash. Physical examination shows a symmetrical rash over the knees and elbows with tense, grouped vesicles, and several excoriation marks. Microabscesses in the papillary dermis are seen on light microscopy. Immunofluorescence shows deposits of immunoglobulin A at the tips of dermal papillae. This patient's skin findings are most likely associated with which of the following?
A 33-year-old woman comes to the physician because of a 14-hour history of left flank pain associated with dark urine. Her temperature is 37.2°C (99°F). The abdomen is soft with normal bowel sounds. There is guarding on the left lateral side and tenderness to palpation over the left costophrenic angle. An x-ray of the abdomen shows an 8-mm kidney stone. Stone analysis reveals a calcium oxalate stone. In addition to adequate hydration, which of the following diets should be advised for this patient?
A 45-year-old woman presents with fever, chills, nausea, and dysuria. She says her symptoms started 4 days ago and have progressively worsened. Her past medical history is significant for recurrent UTIs for the past 6 months and for diabetes mellitus type 2, diagnosed 5 years ago and treated with metformin. Her vital signs include: temperature 39.5°C (103.1°F), blood pressure 100/70 mm Hg, pulse 90/min, and respiratory rate 23/min. On physical examination, moderate right costovertebral angle tenderness is noted. Laboratory findings are significant for the following: WBC 9,500/mm3 RBC 4.20 x 106/mm3 Hematocrit 41.5% Hemoglobin 13.0 g/dL Platelet count 225,000/mm3 Urinalysis: Color Dark yellow Clarity Turbid pH 5.5 Specific gravity 1.021 Glucose None Ketones None Nitrites Positive Leukocyte esterase Positive Bilirubin Negative Urobilirubin 0.6 mg/dL Protein Trace Blood None WBC 25/hpf Bacteria Many Urine culture and sensitivities are pending. Which of the following is the best next step in the management of this patient?
A 36-year-old woman comes to the physician because of a 12-month history of upper abdominal pain. The pain is worse after eating, which she reports as 7 out of 10 in intensity. Over the last year, she has also had nausea, heartburn, and multiple episodes of diarrhea with no blood or mucus. Eight months ago, she underwent an upper endoscopy, which showed several ulcers in the gastric antrum, the pylorus, and the duodenum, as well as thick gastric folds. The biopsies from these ulcers were negative for H. pylori. Current medications include pantoprazole and over-the-counter antacids. She appears anxious. Vital signs are within normal limits. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and there is tenderness to palpation in the epigastric and umbilical areas. Test of the stool for occult blood is positive. A repeat upper endoscopy shows persistent gastric and duodenal ulceration with minimal bleeding. Which of the following is the most appropriate next step in diagnosis?
A 23-year-old woman from Texas is transferred to the intensive care unit after delivering a child at 40 weeks gestation. The pregnancy was not complicated, and there was some blood loss during the delivery. The patient was transferred for severe hypotension refractory to IV fluids and vasopressors. She is currently on norepinephrine and vasopressin with a mean arterial pressure of 67 mmHg. Her past medical history is notable only for a recent bout of asthma treated with albuterol and a prednisone taper over 5 days for contact dermatitis. Physical exam is notable for abnormally dark skin for a Caucasian woman. The patient states she feels extremely weak. However, she did experience breastmilk letdown and was able to breastfeed her infant. Laboratory values are ordered as seen below. Serum: Na+: 127 mEq/L Cl-: 92 mEq/L K+: 6.1 mEq/L HCO3-: 22 mEq/L BUN: 20 mg/dL Creatinine: 1.1 mg/dL Ca2+: 10.2 mg/dL Which of the following is the most likely diagnosis?
A 56-year-old man comes to the physician because of lower back pain for the past 2 weeks. The pain is stabbing and shooting in quality and radiates down the backs of his legs. It began when he was lifting a bag of cement at work. The pain has been getting worse, and he has started to notice occasional numbness and clumsiness while walking. He has hypertension and peripheral artery disease. Medications include hydrochlorothiazide and aspirin. His temperature is 37°C (98.6°F), pulse is 82/min, and blood pressure is 133/92 mm Hg. Peripheral pulses are palpable in all four extremities. Neurological examination shows 5/5 strength in the upper extremities and 3/5 strength in bilateral foot dorsiflexion. Sensation to light touch is diminished bilaterally over the lateral thigh area and the inner side of lower legs. Passive raising of either the right or left leg causes pain radiating down the ipsilateral leg. Which of the following is the most appropriate next step in management?
A 22-year-old woman comes to the emergency department because of chest and epigastric pain that started just after vomiting 30 minutes ago. She does not take any medications and does not drink alcohol or smoke cigarettes. While in the emergency department, the patient experiences two episodes of forceful, bloody emesis. Her temperature is 99.1°F (37.3°C), pulse is 110/minute, and blood pressure is 105/60 mm Hg. Physical examination shows dental enamel erosion and calluses on the dorsal aspect of her right hand. There is tenderness to palpation in the epigastrium. An x-ray of the chest is normal. Further evaluation of this patient is most likely to show which of the following findings?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app