
Gastroenterology — MCQs

On this page
A 28-year-old man presents with one week of redness and discharge in his eyes, pain and swelling in his left second and third toes, and rash on the soles of his feet. He is sexually active with multiple partners and uses condoms occasionally. He denies any recent travel or illness and does not take any medications. Review of systems is otherwise unremarkable. On physical exam, he has bilateral conjunctivitis, dactylitis of the left second and third toes, and crusty yellow-brown vesicles on his plantar feet. Complete blood count and chemistries are within normal limits. Erythrocyte sedimentation rate (ESR) is 40 mm/h. Toe radiographs demonstrate soft tissue swelling but no fractures. Which diagnostic test should be performed next?
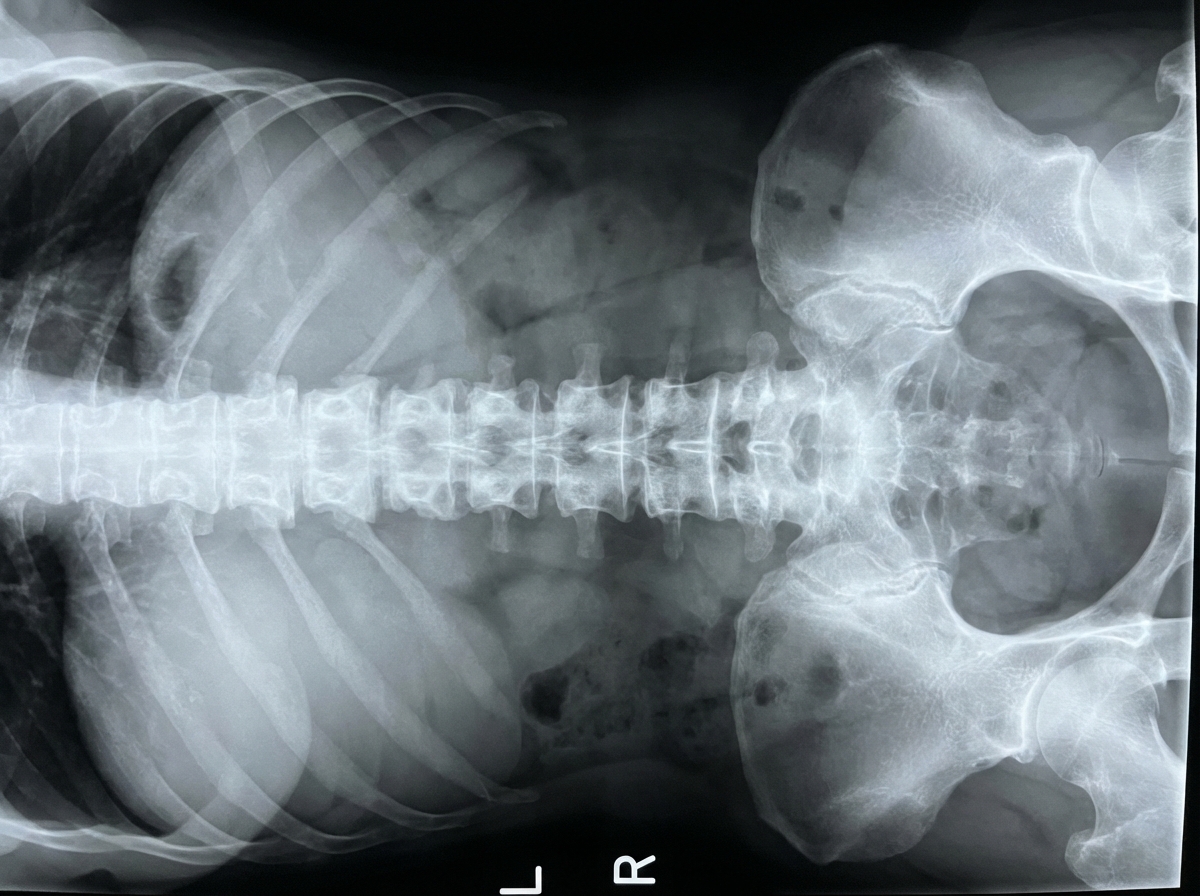
A 32-year-old man presents to the clinic with a dull low back pain radiating to the buttocks. He first noted it about 2 years ago and it has progressed since then. He notes that it is worse in the morning and improves later in the day after physical activity. The patient also reports morning stiffness lasting up to 30 minutes and blurred vision, which started about 7 months ago. The patient's vital signs include: blood pressure 130/80 mm Hg, heart rate 88/min, respiratory rate 16/min, and temperature 36.8°C (98.2°F). Physical examination reveals tenderness over the sacroiliac joints and limitation of the lumbar spine movements in the sagittal plane. The patient's X-ray is shown in the picture below. Which of the following HLA variants is associated with this patient's condition?
A 45-year-old man presents to his primary care physician because of abdominal pain. He has had this pain intermittently for several years but feels that it has gotten worse after he started a low carbohydrate diet. He says that the pain is most prominent in the epigastric region and is also associated with constipation and foul smelling stools that float in the toilet bowl. He has a 15-year history of severe alcoholism but quit drinking 1 year ago. Laboratory studies are obtained showing a normal serum amylase and lipase. Both serum and urine toxicology are negative. His physician starts him on appropriate therapy and checks to make sure that his vitamin and mineral levels are appropriate. Which of the following deficiency syndromes is most closely associated with the cause of this patient's abdominal pain?
A 60-year-old man has had intermittent pain in his right great toe for the past 2 years. Joint aspiration and crystal analysis shows thin, tapered, needle shaped intracellular crystals that are strongly negatively birefringent. Radiograph demonstrates joint space narrowing of the 1st metatarsophalangeal (MTP) joint with medial soft tissue swelling. What is the most likely cause of this condition?
A 67-year-old woman presents to the clinic with a 9-month history of seeing bright red blood in the toilet after defecating. Additional complaints include fatigue, shortness of breath, and mild lethargy. She denies the loss of weight, abdominal pain, or changes in dietary behavior. She consumes a balanced diet and takes multiple vitamins every day. The current vital signs include the following: temperature is 37.0°C (98.6°F), pulse rate is 68/min, blood pressure is 130/81 mm Hg, and the respiratory rate is 13/min. On physical examination, you notice increased capillary refill time and pale mucosa. What are the most likely findings for hemoglobin, hematocrit, red blood cell count, and mean corpuscular volume?
A 35-year-old woman presents for evaluation of symmetric proximal muscle weakness. The patient also presents with a blue-purple discoloration of the upper eyelids accompanied by rashes on the knuckles, as shown in the picture below. What is the most likely cause?

A 34-year-old female with a past medical history of a gastric sleeve operation for morbid obesity presents for pre-surgical clearance prior to a knee arthroplasty. Work-up reveals a hemoglobin of 8.7 g/dL, hematocrit of 26.1%, and MCV of 106 fL. With concern for folate deficiency, she is started on high dose folate supplementation, and her follow-up labs are as follows: hemoglobin of 10.1 g/dL, hematocrit of 28.5%, and MCV of 96 fL. Given her history of gastric sleeve surgery and associated malabsorption risks, she is at long-term risk for which complication?
A 44-year-old man comes to the physician because of progressive memory loss for the past 6 months. He reports that he often misplaces his possessions and has begun writing notes to remind himself of names and important appointments. He generally feels fatigued and unmotivated, and has poor concentration at work. He has also given up playing soccer because he feels slow and unsteady on his feet. He has also had difficulty swallowing food over the last two weeks. His temperature is 37.8°C (100°F), pulse is 82/min, respirations are 16/min, and blood pressure is 144/88 mm Hg. Examination shows confluent white plaques on the posterior oropharynx. Neurologic examination shows mild ataxia and an inability to perform repetitive rotary forearm movements. Mental status examination shows a depressed mood and short-term memory deficits. Serum glucose, vitamin B12 (cyanocobalamin), and thyroid-stimulating hormone concentrations are within the reference range. Upper esophagogastroduodenoscopy shows streaky, white-grayish lesions. Which of the following is the most likely underlying cause of this patient's neurological symptoms?
A 57-year-old man presents with 2 days of severe, generalized, abdominal pain that is worse after meals. He is also nauseated and reports occasional diarrhea mixed with blood. Apart from essential hypertension, his medical history is unremarkable. His vital signs include a temperature of 36.9°C (98.4°F), blood pressure of 145/92 mm Hg, and an irregularly irregular pulse of 105/min. Physical examination is only notable for mild periumbilical tenderness. Which of the following is the most likely diagnosis?
A 46-year-old man presents with increasing fatigue and weakness for the past 3 months. He works as a lawyer and is handling a complicated criminal case which is very stressful, and he attributes his fatigue to his work. He lost 2.3 kg (5.0 lb) during this time despite no change in diet or activity level. His past history is significant for chronic constipation and infrequent episodes of bloody stools. Family history is significant for his father and paternal uncle who died of colon cancer and who were both known to possess a genetic mutation for the disease. He has never had a colonoscopy or had any genetic testing performed. Physical examination is significant for conjunctival pallor. A colonoscopy is performed and reveals few adenomatous polyps. Histopathologic examination shows high-grade dysplasia and genetic testing reveals the same mutation as his father and uncle. The patient is concerned about his 20-year-old son. Which of the following is the most appropriate advice regarding this patient's son?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app