
Gastroenterology — MCQs

On this page
A 36-year-old man presents with soreness and dryness of the oral mucosa for the past 3 weeks. No significant past medical history. The patient reports that he has had multiple bisexual partners over the last year and only occasionally uses condoms. He denies any alcohol use or history of smoking. The patient is afebrile and his vital signs are within normal limits. On physical examination, there is a lesion noted in the oral cavity, which is shown in the exhibit. Which of the following is the next best step in the treatment of this patient?

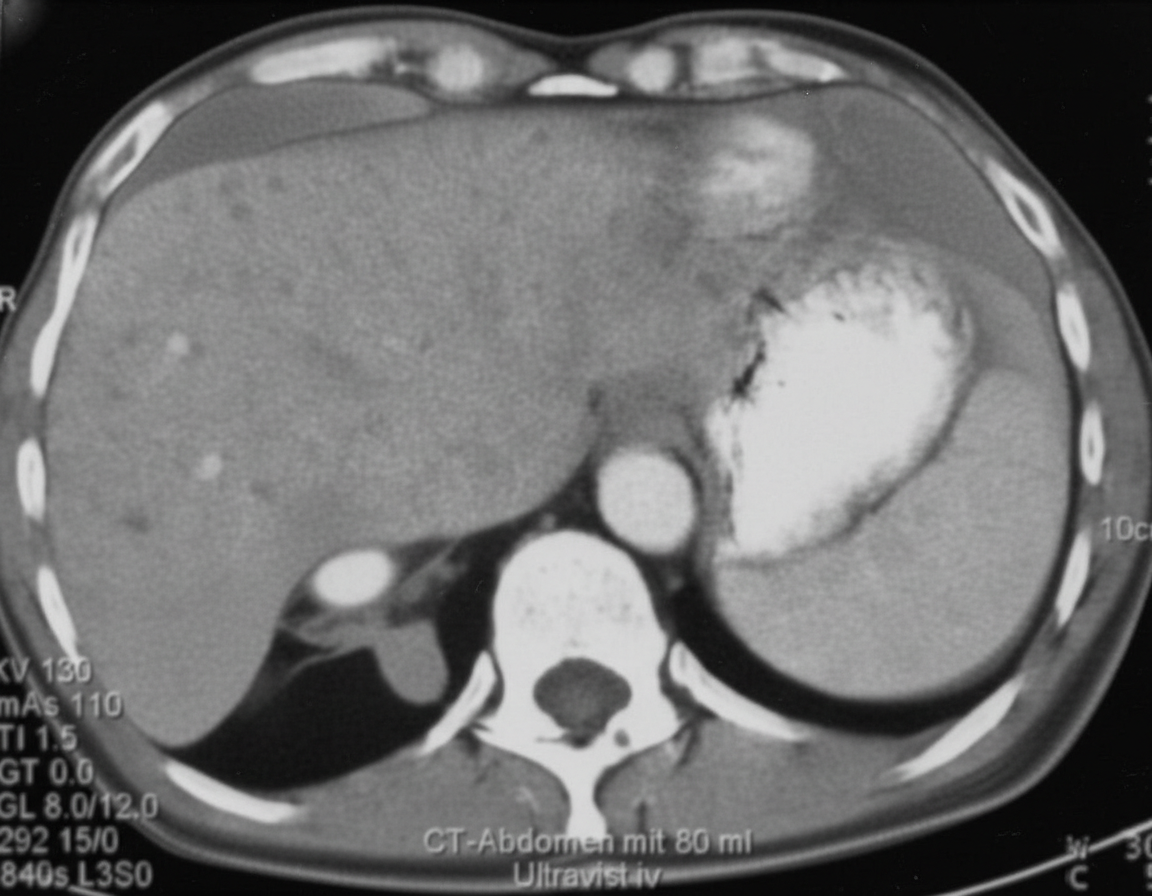
A 64-year-old woman comes to the physician because of a 7.2-kg (16-lb) weight loss over the past 6 months. For the last 4 weeks, she has also had intermittent constipation and bloating. Four months ago, she spent 2 weeks in Mexico with her daughter. She has never smoked. She drinks one glass of wine daily. She appears thin. Her temperature is 38.3°C (101°F), pulse is 80/min, and blood pressure is 136/78 mm Hg. The lungs are clear to auscultation. The abdomen is distended and the liver is palpable 4 cm below the right costal margin with a hard, mildly tender nodule in the left lobe. Test of the stool for occult blood is positive. Serum studies show: Alkaline phosphatase 67 U/L AST 65 U/L ALT 68 U/L Hepatitis B surface antigen negative Hepatitis C antibody negative A contrast-enhanced CT scan of the abdomen is shown. Which of the following is the most likely diagnosis?
A 76-year-old man presents after an acute onset seizure. He lives in a retirement home and denies any previous history of seizures. Past medical history is significant for a hemorrhagic stroke 4 years ago, and type 2 diabetes, managed with metformin. His vital signs include: blood pressure 80/50 mm Hg, pulse 80/min, and respiratory rate 19/min. On physical examination, the patient is lethargic. Mucous membranes are dry. A noncontrast CT of the head is performed and is unremarkable. Laboratory findings are significant for the following: Plasma glucose 680 mg/dL pH 7.37 Serum bicarbonate 17 mEq/L Effective serum osmolality 350 mOsm/kg Urinary ketone bodies negative Which of the following was the most likely trigger for this patient’s seizure?
A 70-year-old woman is brought to the emergency department 1 hour after being found unconscious in her apartment by her neighbor. No medical history is currently available. Her temperature is 37.2°C (99.0°F), pulse is 120/min, respirations are 18/min, and blood pressure is 70/50 mm Hg. Physical examination reveals dry mucous membranes and poor skin turgor. The neighbor mentions that the patient had been complaining of severe diarrhea for the past 2 days. Laboratory studies show a glomerular filtration rate of 70 mL/min/1.73 m2 (N > 90) and an increased filtration fraction. Which of the following is the most likely cause of this patient's findings?
A 24-year-old woman with 45,X syndrome comes to the physician because of diarrhea for 4 months. She also reports bloating, nausea, and abdominal discomfort that persists after defecation. For the past 6 months, she has felt tired and has been unable to do her normal chores. She went on a backpacking trip across Southeast Asia around 7 months ago. She is 144 cm (4 ft 9 in) tall and weighs 40 kg (88 lb); BMI is 19 kg/m2. Her blood pressure is 110/60 mm Hg in the upper extremities and 80/40 mm Hg in the lower extremities. Examination shows pale conjunctivae and angular stomatitis. Abdominal examination is normal. Laboratory studies show: Hemoglobin 9.1 mg/dL Leukocyte count 5100/mm3 Platelet count 200,000/mm3 Mean corpuscular volume 67 μmm3 Serum Na+ 136 mEq/L K+ 3.7 mEq/L Cl- 105 mEq/L Glucose 89 mg/dL Creatinine 1.4 mg/dL Ferritin 10 ng/mL IgA tissue transglutaminase antibody positive Based on the laboratory studies, a biopsy for confirmation of the diagnosis is suggested, but the patient is unwilling to undergo the procedure. Which of the following is the most appropriate next step in management of this patient's gastrointestinal symptoms?
A 30-year-old male visits you in the clinic complaining of chronic abdominal pain and diarrhea following milk intake. Gastrointestinal histology of this patient's condition is most similar to which of the following?
A 41-year-old man presents to the emergency department because of brownish discoloration of his urine for the last several days. The review of symptoms includes complaints of increasing abdominal girth, early satiety, and difficulty breathing on exertion. The past medical history includes essential hypertension for 19 years. The medication list includes lisinopril and hydrochlorothiazide. He had a right inguinal hernia repair when he was a teenager. He smokes 20–30 cigarettes daily for the last 21 years, and drinks alcohol socially. His father died of a hemorrhagic stroke at the age of 69 years. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 131/88 mm Hg, and pulse 82/min. The physical examination is positive for a palpable right upper quadrant mass. The abdominal ultrasound shows multiple bilateral kidney cysts and hepatic cysts. Which of the following is the most likely diagnosis?
A 75-year-old man comes to the physician because of a 3-month history of upper abdominal pain, nausea, and sensation of early satiety. He has also had a 9.4-kg (20.7-lb) weight loss over the past 4 months. He has osteoarthritis. He drinks two beers every night with dinner. His only medication is ibuprofen. Esophagogastroduodenoscopy shows an ulcerated mass in the lesser curvature of the stomach. A biopsy specimen obtained during endoscopy shows irregular-shaped tubules with intraluminal mucus and debris. Which of the following is the most likely predisposing factor for this patient's condition?
A 72-year-old male with a past medical history significant for aortic stenosis and hypertension presents to the emergency department complaining of weakness for the past 3 weeks. He states that, apart from feeling weaker, he also has noted lightheadedness, pallor, and blood-streaked stools. The patient's vital signs are stable, and he is in no acute distress. Laboratory workup reveals that the patient is anemic. Fecal occult blood test is positive for bleeding. EGD was performed and did not reveal upper GI bleeding. Suspecting a lower GI bleed, a colonoscopy is performed after prepping the patient, and it is unremarkable. What would be an appropriate next step for localizing a lower GI bleed in this patient?
A 53-year-old woman is brought to the emergency department because of an episode of lightheadedness and left arm weakness for the last hour. Her symptoms were preceded by tremors, palpitations, and diaphoresis. During the past 3 months, she has had increased appetite and has gained 6.8 kg (15 lbs). She has hypertension, hyperlipidemia, anxiety disorder, and gastroesophageal reflux. She works as a nurse in an ICU and has been under more stress than usual. She does not smoke. She drinks 5 glasses of wine every week. Current medications include enalapril, atorvastatin, fluoxetine, and omeprazole. She is 168 cm (5 ft 6 in) tall and weighs 100 kg (220 lb); BMI is 36 kg/m2. Her temperature is 37°C (98.8°F), pulse is 78/min, and blood pressure is 130/80 mm Hg. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and nontender. Fasting serum studies show: Na+ 140 mEq/L K+ 3.5 mEq/L HCO3- 22 mEq/L Creatinine 0.8 mg/dL Glucose 37 mg/dL Insulin 280 μU/mL (N=11–240) Thyroid-stimulating hormone 2.8 μU/mL C-peptide 4.9 ng/mL (N=0.8–3.1) Urine screen for sulfonylurea is negative. Which of the following is the most likely diagnosis?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app