
Gastroenterology — MCQs

On this page
A 45-year-old man comes to the physician because of a 5-day history of fever, malaise, and right upper abdominal pain. Examination of the abdomen shows tenderness in the right upper quadrant. His leukocyte count is 18,000/mm3 (90% neutrophils) and serum alkaline phosphatase is 130 U/L. Ultrasonography of the abdomen shows a 3-cm hypoechoic lesion in the right lobe of the liver with a hyperemic rim. Which of the following is the most likely underlying cause of this patient's condition?
A 40-year-old woman presents with a lack of concentration at work for the last 3 months. She says that she has been working as a personal assistant to a manager at a corporate business company for the last 2 years. Upon asking why she is not able to concentrate, she answers that her colleagues are always gossiping about her during work hours and that it disrupts her concentration severely. Her husband works in the same company and denies these allegations. He says the other employees are busy doing their own work and have only formal conversations, yet she is convinced that they are talking about her. He further adds that his wife frequently believes that some advertisements in a newspaper are directed towards her and are published specifically to catch her attention even though they are routine advertisements. The patient denies any mood disturbances, anxiety or hallucinations. Past medical history is significant for a tingling sensation in her legs, 3+ patellar reflexes bilaterally, and absent ankle reflexes bilaterally. She says that she drinks alcohol once to twice a month for social reasons but denies any other substance use or smoking. On physical examination, the patient is conscious, alert, and oriented to time, place and person. A beefy red color of the tongue is noted. No associated cracking, bleeding, or oral lesions. Which of the following laboratory tests would be most helpful to identify this patient’s most likely diagnosis?
A 23-year-old man comes to the physician for frequent and painful urination. He has also had progressive painful swelling of his right knee over the past week. He is sexually active with two female partners and uses condoms inconsistently. His mother has an autoimmune disease that involves a malar rash. Examination shows conjunctivitis bilaterally. The right knee is warm, erythematous, and tender to touch; range of motion is limited. Laboratory studies show an erythrocyte sedimentation rate of 62 mm/h. Urinalysis shows WBCs. Further evaluation of this patient is most likely to reveal which of the following?
A 74-year-old man is brought to the emergency department after he had copious amounts of blood-stained stools. Minutes later, he turned sweaty, felt light-headed, and collapsed into his wife’s arms. Upon admission, he is found to have a blood pressure of 78/40 mm Hg, a pulse of 140/min, and oxygen saturation of 98%. His family history is relevant for both gastric and colorectal cancer. His personal history is relevant for hypertension, for which he takes amlodipine. After an initial successful resuscitation with intravenous fluids, which of the following should be the first step in approaching this case?
A 27-year-old man presents with a 2-week history of fever, malaise, and occasional diarrhea. On physical examination, the physician notes enlarged inguinal lymph nodes. An HIV screening test is positive. Laboratory studies show a CD4+ count of 650/mm3. This patient is most likely currently in which of the following stages of HIV infection?
A 40-year-old overweight man presents to the office complaining of heartburn for 6 months. He describes burning in his chest brought on by meals. He has a 20 pack-year smoking history and drinks 2 glasses of red wine with dinner nightly. He denies dysphagia, odynophagia, weight loss, melena, and hematemesis. Over the past month, he has reduced his intake of fatty and spicy foods with some moderate relief of his symptoms; however, his symptoms are still present. He also has stopped smoking. Which of the following is the most appropriate next step in the care of this patient?
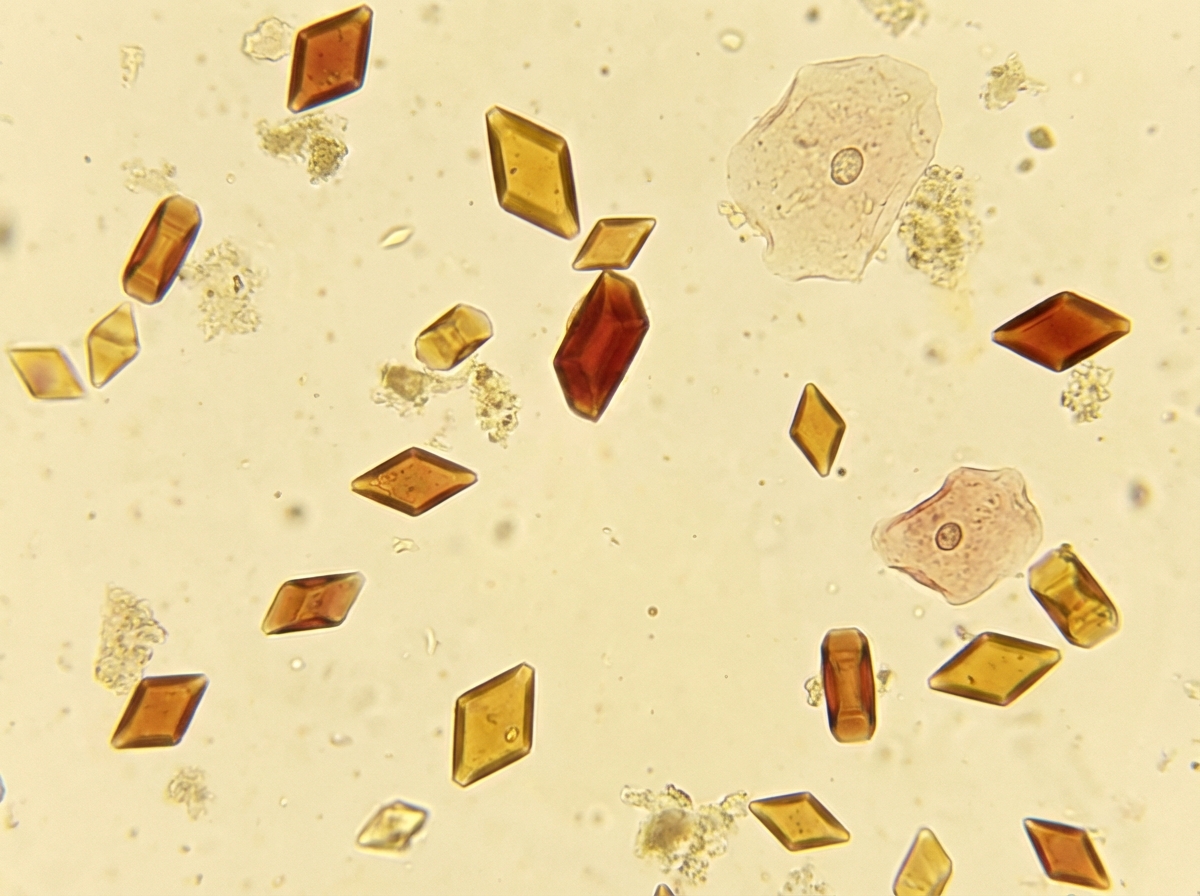
A 23-year-old man presents to the emergency room with right flank pain. On physical examination, there is no rebound tenderness, guarding, and rigidity. The pain is radiating to the groin region and is associated with nausea. Plain X-ray of the kidney, ureter, and bladder is normal. Urinalysis showed the presence of mild hematuria, an absence of pus cells, and the following crystals (refer to image). What is the most likely composition of these crystals?
A 27-year-old man presents to his primary care physician after a recent illness. For the past 48 hours the patient has experienced constant vomiting and diarrhea with a high fever. He is feeling better today and wants to be seen to ensure he is healthy. The patient has a past medical history of schizophrenia well controlled with risperidone and lithium. He takes ibuprofen for knee pain and attempts to stay well hydrated. Laboratory values are ordered as seen below. Serum: Na+: 123 mEq/L Cl-: 90 mEq/L K+: 3.8 mEq/L HCO3-: 29 mEq/L BUN: 42 mg/dL Glucose: 109 mg/dL Creatinine: 1.9 mg/dL Ca2+: 10.2 mg/dL Which of the following is the most likely explanation for this patient’s laboratory derangements?
An 18-year-old man presents to his primary care provider before leaving for college. He has no complaints. His past medical history is significant for asthma, acne vulgaris, and infectious mononucleosis at age 16. His home medications include doxycycline and albuterol as needed. His family history is significant for colon cancer in his father at age 50, his paternal grandfather at age 55, and an uncle at age 45. His father underwent testing for mutations in the APC gene, which were negative. There is no family history of dental abnormalities or other malignancy. The patient denies any recent weight loss, abdominal pain, hematochezia, melena, or other changes in the appearance of his stools. This patient should be screened for colorectal cancer (CRC) under which of the following protocols?
A 55-year-old woman presents to the emergency department with retrosternal pain that started this evening. The patient states that her symptoms started as she was going to bed after taking her medications. She describes the pain as sudden in onset, worse with swallowing, and not associated with exertion. The patient has a past medical history of diabetes, anemia, and congestive heart failure and is currently taking metoprolol, insulin, metformin, iron, and lisinopril. Her temperature is 99.2°F (37.3°C), blood pressure is 125/63 mmHg, pulse is 90/min, respirations are 14/min, and oxygen saturation is 100% on room air. Physical exam is notable for an obese woman who appears uncomfortable. An initial electrocardiogram (ECG) demonstrates sinus rhythm, and a set of troponins are pending. Which of the following is the most likely diagnosis?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app