
Gastroenterology — MCQs

On this page
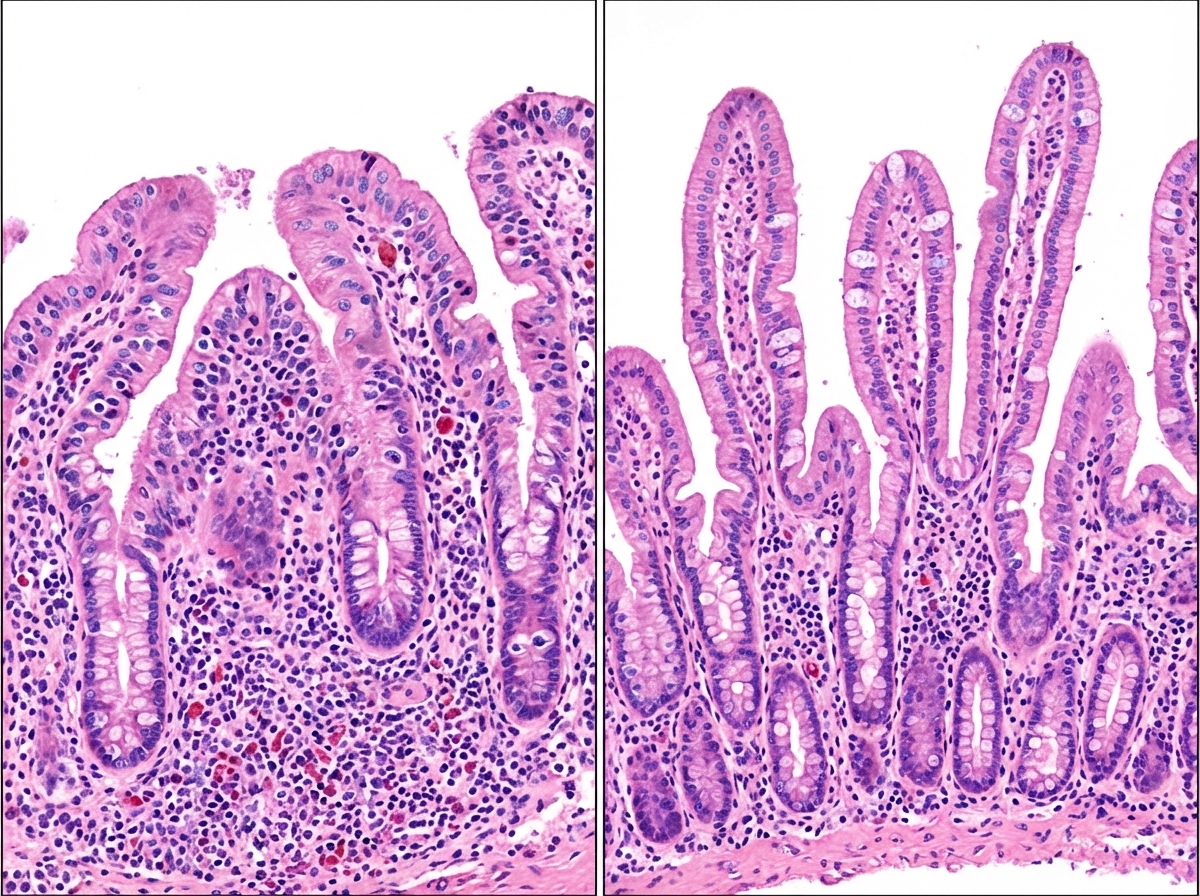
Compare the intestinal biopsy specimen of patient before and after diet restriction. All are true about the condition shown except:
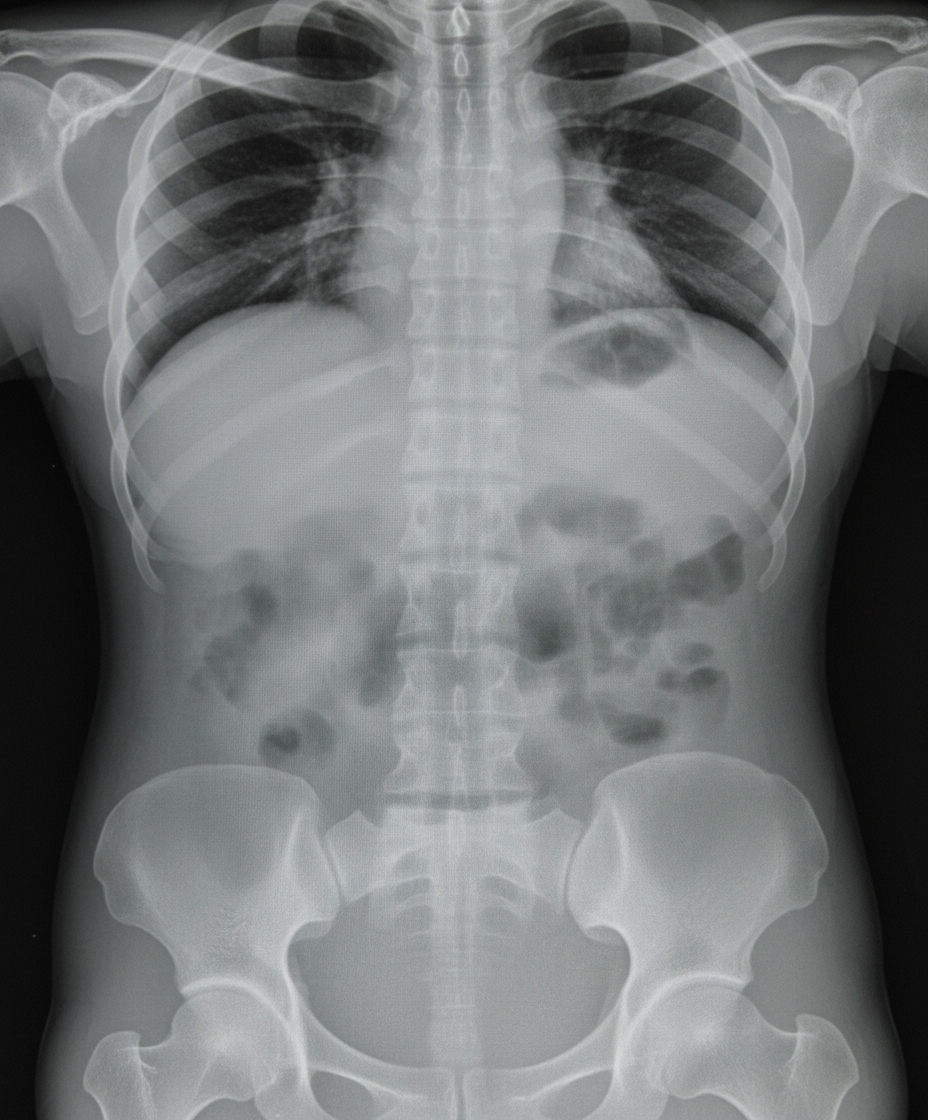
A patient presents with complaints of fever and abdominal distention. He is having history of bloody diarrhea off and on for previous 6 months. X-ray abdomen is shown below. What is the diagnosis?
A 38-year-old patient complains of rectal bleeding, tenesmus and mucous discharge. On examination patient is found to have anemia, hypoproteinemia and electrolyte disturbance. On radiological examination this is the presentation of the patient. Which of the following statement is false?

A patient presents with itchy skin lesions with blistering along with gastrointestinal issues. Which of the following is the most specific serological test for this condition?
An adult female presents with pallor and fatigue. Blood investigations show low hemoglobin ( Hb ), low serum iron, low ferritin, low transferrin saturation, and increased total iron-binding capacity (TIBC). What is the likely diagnosis?
Which of the following is typically observed in the investigation results for a patient with iron deficiency anemia (IDA)?
Which of the following antibodies is associated with Celiac disease?
An endoscopic image shows the following finding. What is the most likely diagnosis?

A female engineer works for 12-14 hours a day and reports consuming only fast food, with no vegetables or fruits in her diet. Her hemoglobin (Hb) count is $9 \mathrm{~g} / \mathrm{dL}$, and her mean corpuscular volume (MCV) is 120 fL . Peripheral smear (PS) shows the presence of macrocytes. What is the most likely diagnosis?
A 71-year-old man presents to the emergency department because of blood in his stool. The patient states that he is not experiencing any pain during defecation and is without pain currently. The patient recently returned from a camping trip where he consumed meats cooked over a fire pit and drank water from local streams. The patient has a past medical history of obesity, diabetes, constipation, irritable bowel syndrome, ulcerative colitis that is in remission, and a 70 pack-year smoking history. The patient has a family history of breast cancer in his mother and prostate cancer in his father. His temperature is 98.9°F (37.2°C), blood pressure is 160/87 mmHg, pulse is 80/min, respirations are 14/min, and oxygen saturation is 98% on room air. Physical exam is notable for an obese man in no current distress. Abdominal exam reveals a non-tender and non-distended abdomen with normal bowel sounds. An abdominal radiograph and barium swallow are within normal limits. Assuming appropriate diagnostic workup identifies the most likely cause of his symptoms, which of the following would be the most appropriate treatment?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app