
Gastroenterology — MCQs

On this page
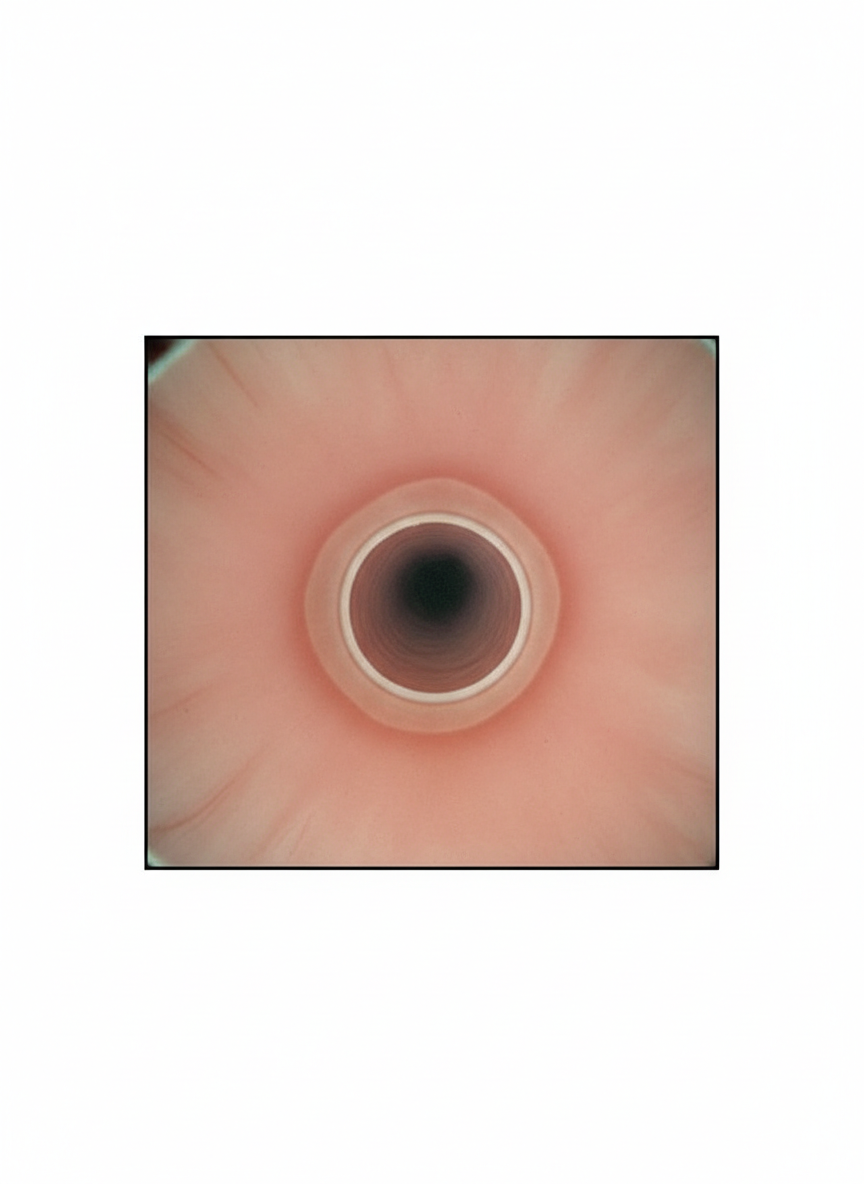
A 45-year-old man presents to an ambulatory clinic for evaluation after feeling food stuck behind the sternum when he was eating a hamburger last night. He was not in pain. He had to drink a whole glass of water to get the food down; however, he did manage to finish his dinner without any further problems. He is concerned because he has had 2 similar episodes this year. He is otherwise healthy. He has smoked 1 half-pack of cigarettes a day for 20 years and enjoys a can of beer every night. His vital signs are as follows: blood pressure 125/75 mm Hg, pulse 68/min, respiratory rate 14/min, and temperature 36.5°C (97.7°F). His oral examination reveals 2 decayed teeth. The physical exam is otherwise unremarkable. An endoscopic image of the lower esophagus is shown. Which of the following is the most appropriate next step in management?
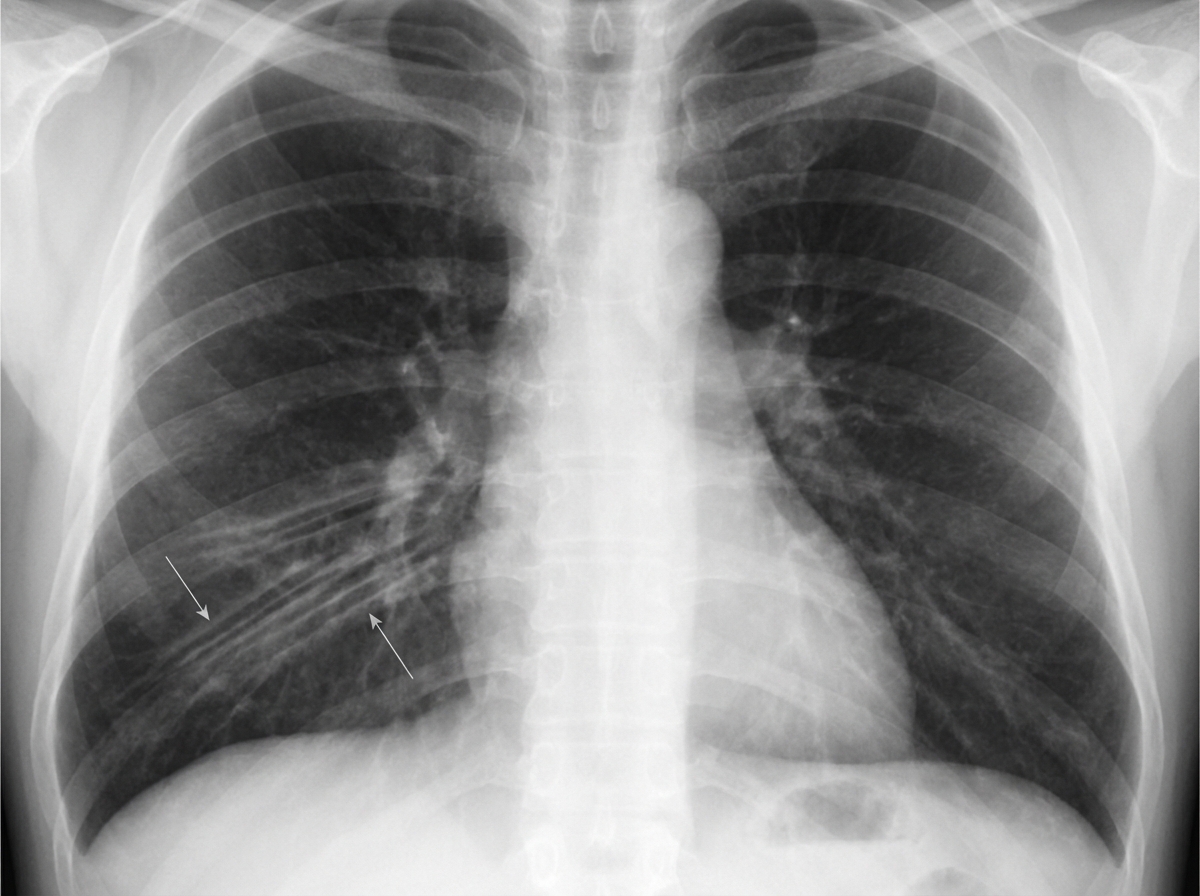
A 65-year-old man is brought to the emergency department after coughing up copious amounts of blood-tinged sputum at his nursing home. He recently had an upper respiratory tract infection that was treated with antibiotics. He has a long-standing history of productive cough that has worsened since he had a stroke 3 years ago. He smoked a pack of cigarettes daily for 40 years until the stroke, after which he quit. The patient appears distressed and short of breath. His temperature is 38°C (100.4°F), pulse is 92/min, and blood pressure is 145/85 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 92%. Physical examination shows digital clubbing and cyanosis of the lips. Coarse crackles are heard in the thorax. An x-ray of the chest shows increased translucency and tram-track opacities in the right lower lung field. Which of the following is the most likely diagnosis?
A 57-year-old woman comes to the physician because of a 3-month history of easy fatigability and dyspnea on exertion. Menopause occurred 5 years ago. Her pulse is 105/min and blood pressure is 100/70 mm Hg. Physical examination shows pallor of the nail beds and conjunctivae. A peripheral blood smear shows small, pale red blood cells. Further evaluation is most likely to show which of the following findings?
A 31-year old man presents to the emergency department for blood in his stool. The patient states that he saw a small amount of bright red blood on his stool and on the toilet paper this morning, which prompted his presentation to the emergency department. The patient denies any changes in his bowel habits or in his weight. The patient has a past medical history of asthma managed with albuterol and fluticasone. The patient has a family history of alcoholism in his father and suicide in his mother. His temperature is 97°F (36.1°C), blood pressure is 120/77 mmHg, pulse is 60/min, respirations are 12/min, and oxygen saturation is 98% on room air. On physical exam, the patient has a cardiac and pulmonary exam that are within normal limits. On abdominal exam, there is no tenderness or guarding and normal bowel sounds. Laboratory values are ordered and return as below. Hemoglobin: 15 g/dL Hematocrit: 42% Leukocyte count: 4,500 cells/mm^3 with normal differential Platelet count: 230,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 24 mEq/L BUN: 20 mg/dL Glucose: 92 mg/dL Creatinine: 1.0 mg/dL Ca2+: 9.9 mg/dL Which of the following is the next best step in management?
A 25-year-old man comes to the physician because of a 4-day history of bloody stools. During this time, he has not had nausea, vomiting, abdominal cramps, or pain while defecating. He has had recurrent episodes of non-bloody diarrhea for the past 6 months. His father died of colon cancer at the age of 39 years. His vital signs are within normal limits. Physical examination shows small, painless bony swellings on the mandible, forehead, and right shin. There are multiple non-tender, subcutaneous nodules with central black pores present over the trunk and face. Fundoscopic examination shows multiple, oval, darkly pigmented lesions on the retina. Colonoscopy shows approximately 150 colonic polyps. Which of the following is the most likely diagnosis?
An 18-year-old woman comes to see her primary care physician for a physical for school. She states she has not had any illnesses last year and is on her school's volleyball team. She exercises daily, does not use any drugs, and has never smoked cigarettes. On physical exam you note bruising around the patients neck, and what seems to be burn marks on her back and thighs. The physician inquires about these marks. The patient explains that these marks are the result of her sexual activities. She states that in order for her to be aroused she has to engage in acts such as hitting, choking, or anything else that she can think of. The physician learns that the patient lives with her boyfriend and that she is in a very committed relationship. She is currently monogamous with this partner. The patient is studying with the hopes of going to law school and is currently working in a coffee shop. The rest of the patient’s history and physical is unremarkable. Which of the following is the most likely diagnosis?
A 57-year-old woman presents to her primary care physician with a chief complaint of epigastric pain that has worsened over the past three weeks. She describes it as sudden “gnawing” sensations that last for up to half a minute before subsiding. She finds some relief after a glass of water, but does not associate relief or exacerbation around mealtimes. The patient denies any radiation of the pain, fever, weight loss, fatigue, or change in stool color and quality. She does not take any medications, and says her diet includes lots of spicy and smoked foods. The physician refers her for an upper endoscopy, which reveals evidence of duodenal ulcers and mild gastroesophageal reflux. The pathology report reveals focal intestinal metaplasia and gastric dysplasia in the stomach, but no Helicobacter pylori infection. How should the physician advise this patient?
A 60-year-old man comes to the emergency department because of recurrent episodes of fatigue, palpitations, nausea, and diaphoresis over the past 6 months. The episodes have become more frequent in the last 2 weeks and he has missed work several times because of them. His symptoms usually improve after he drinks some juice and rests. He has had a 2-kg (4.5-lb) weight gain in the past 6 months. He has a history of bipolar disorder, hypertension, and asthma. His sister has type 2 diabetes mellitus and his mother has a history of medullary thyroid carcinoma. His medications include lithium, hydrochlorothiazide, aspirin, and a budesonide inhaler. His temperature is 36.3°C (97.3°F), pulse is 92/min and regular, respirations are 20/min, and blood pressure is 118/65 mm Hg. Abdominal examination shows no abnormalities. Serum studies show: Na+ 145 mEq/L K+ 3.9 mEq/L Cl- 103 mEq/L Calcium 9.2 mg/dL Glucose 88 mg/dL Which of the following is the most appropriate next step in diagnosis?
A 34-year-old man presents with dysphagia. The patient says that he has pain on swallowing which gradually onset 2 weeks ago and has not improved. He denies any change in diet but does say that he recently returned from a prolonged work trip to the Caribbean. No significant past medical history or current medications. On physical examination, the patient looks pale. His tongue is swollen and has a beefy, red appearance. Angular stomatitis is present. Laboratory findings are significant for macrocytic, megaloblastic anemia, decreased serum folate, increased serum homocysteine, and normal methylmalonic acid levels. Which of the following conditions most likely caused this patient’s symptoms?
A 45-year-old woman presents to the clinic complaining of weakness that has progressively worsened over the past 2 weeks. She states that she has a hard time lifting both her arms but that they function normally. She notes no history of trauma or other deficits. On examination, that patient has 2/5 muscle strength on shoulder shrug and arm abduction bilaterally, but all other neurological exam findings are normal. You notice some skin changes and ask the patient about them. She states that she has had a rash around her eyes as well as on her lower face, going down to her neck and chest. She notes that the rashes started around the same time as the weakness began. Labs are drawn and a complete blood count and basic metabolic panel are normal. Which of the following is the most likely diagnosis?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app