
Gastroenterology — MCQs

On this page
A 48-year-old man comes to the physician because of severe joint pain and swelling involving different joints for 3 months. He has also been having loose stools and episodes of epigastric pain for 6 months. He reports a 10-kg (22-lb) weight loss during this period. He has type 2 diabetes mellitus. He does not smoke or drink alcohol. His medications include insulin and metformin. His vital signs are within normal limits. Examination shows pale conjunctivae, angular cheilitis, and glossitis. Axillary and cervical lymphadenopathy is present. A grade 2/6 pansystolic murmur is heard best at the apex. The right knee is swollen and tender; range of motion is limited. The sacroiliac joints are tender. Test of the stool for occult blood is negative. Laboratory studies show: Hemoglobin 9.2 g/dL Mean corpuscular volume 90 μm3 Leukocyte count 4,800/mm3 Serum Na+ 134 mEq/L Cl- 96 mEq/L K+ 3.3 mEq/L Glucose 143 mg/dL Creatinine 1.2 mg/dL A small intestine biopsy shows periodic acid-Schiff-positive (PAS-positive) macrophages in the lamina propria. Which of the following is the most appropriate next step in management?
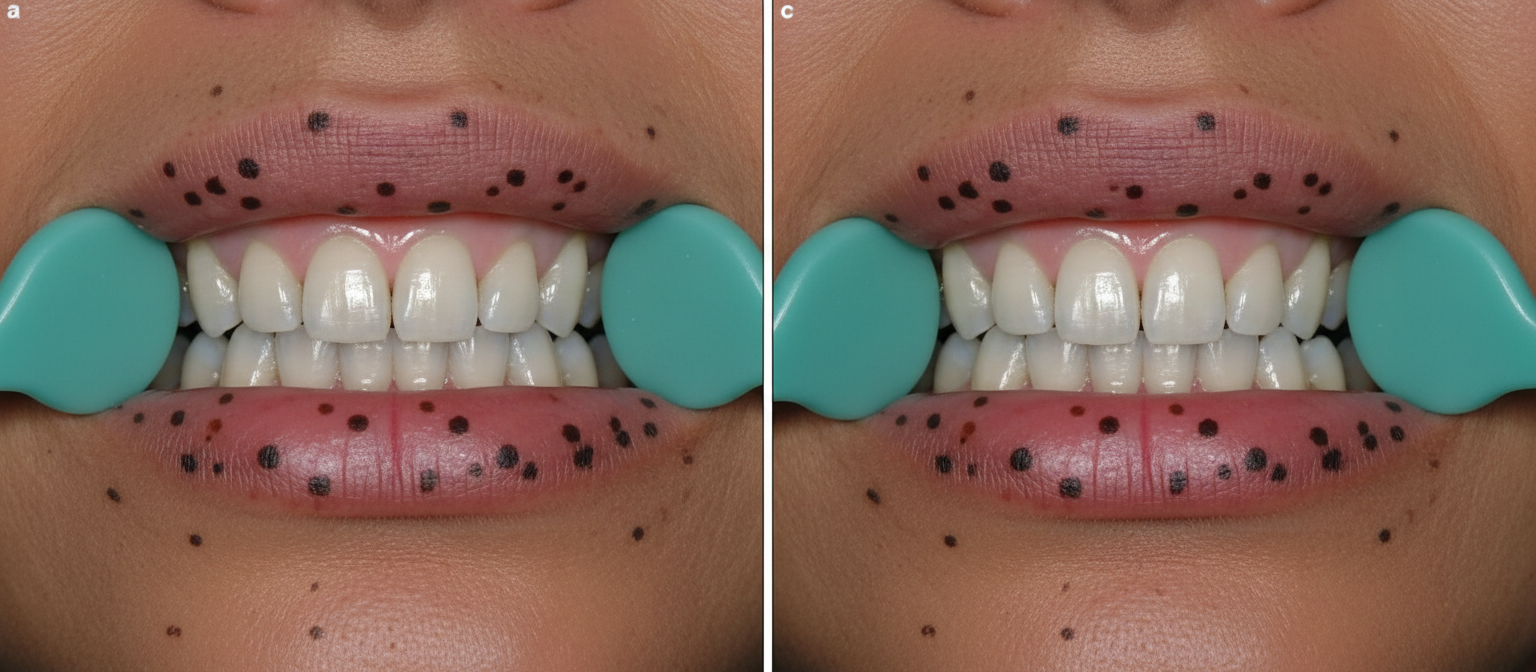
A 39-year-old woman comes to the physician for a follow-up examination after a colonoscopy showed 42 hamartomatous polyps. The physical examination findings are shown in the photograph. Which of the following conditions is most likely to develop in this patient?
A 45-year-old obese woman presents to the office complaining of intermittent chest pain for the past 3 days. She states that the pain worsens when she lays down and after she eats her meals. She thinks that she has experienced similar pain before but does not remember it lasting this long. She also complains of a bitter taste in her mouth but is otherwise in no apparent distress. She has a history of asthma, a partial hysterectomy 4 years ago, and hypothyroidism that was diagnosed 7 years ago. She admits to drinking 5–6 cans of beer on weekend nights. Her blood pressure is 130/90 mm Hg, and her heart rate is 105/min. An ECG is performed that shows no abnormal findings. Which of the following is the most likely cause of her pain?
A previously healthy 37-year-old man comes to the physician for the evaluation of an 8-week history of intermittent burning epigastric pain. During this period, he has also felt bloated and uncomfortable after meals. He has not had weight loss or a change in bowel habits. He has no personal or family history of serious illness. He takes no medications. He does not smoke. He drinks 1–3 beers per week. Vital signs are within normal limits. Abdominal examination shows mild epigastric tenderness on palpation without guarding or rebound tenderness. Bowel sounds are normal. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?
A 59-year-old man comes to the emergency department because of worsening nausea and reduced urine output for the past 3 days. One week ago he had a 4-day episode of abdominal pain, vomiting, and watery, nonbloody diarrhea that began a day after he returned from a trip to Mexico. He has not been able to eat or drink much since then, but the symptoms resolved 3 days ago. He has a history of tension headaches, for which he takes ibuprofen about 10 times a month. He also has gastroesophageal reflux disease and benign prostatic hyperplasia. His daily medications include pantoprazole and alfuzosin. He appears pale. His temperature is 36.9°C (98.4°F), pulse is 120/min, and blood pressure is 90/60 mm Hg. Examination shows dry mucous membranes. The abdomen is soft without guarding or rebound. Laboratory studies show: Hemoglobin 14.8 g/dL Platelet count 250,000/mm3 Serum Na+ 147 mEq/L Cl- 102 mEq/L K+ 4.7 mEq/L HCO3- 20 mEq/L Urea nitrogen 109 mg/dL Glucose 80 mg/dL Creatinine 3.1 mg/dL Urinalysis shows no abnormalities. Which of the following is the most likely underlying cause of this patient's laboratory findings?
A 63-year-old woman comes to the physician for evaluation of worsening fatigue and an unintentional 6.8-kg (15-lb) weight loss over the past 2 months. She also reports having had an unusual appetite for soil and clay for several months. She has a history of osteoarthritis of the knees, for which she takes acetaminophen. Her pulse is 116/minute and blood pressure is 125/84 mm Hg. Physical examination shows diffuse teeth abrasions and dirt in the sublingual folds. Further evaluation of this patient is most likely to show which of the following findings?
A 45-year-old woman comes to the physician because of a 5-month history of recurrent retrosternal chest pain that often wakes her up at night. Physical examination shows no abnormalities. Upper endoscopy shows hyperemia in the distal third of the esophagus. A biopsy specimen from this area shows non-keratinized stratified squamous epithelium with hyperplasia of the basal cell layer and neutrophilic inflammatory infiltrates. Which of the following is the most likely underlying cause of this patient's findings?
A 31-year-old man comes to the physician because of worsening abdominal pain, an inability to concentrate at work, and a general lack of motivation over the past several months. He has a history of spontaneous passage of two kidney stones. His father and uncle underwent thyroidectomy before the age of 35 for thyroid cancer. Physical examination shows diffuse tenderness over the abdomen. Serum studies show: Na+ 142 mEq/L K+ 3.7 mEq/L Glucose 131 mg/dL Ca2+ 12.3 mg/dL Albumin 4.1 g/dL Parathyroid hormone 850 pg/mL Further evaluation is most likely to show elevated levels of which of the following?
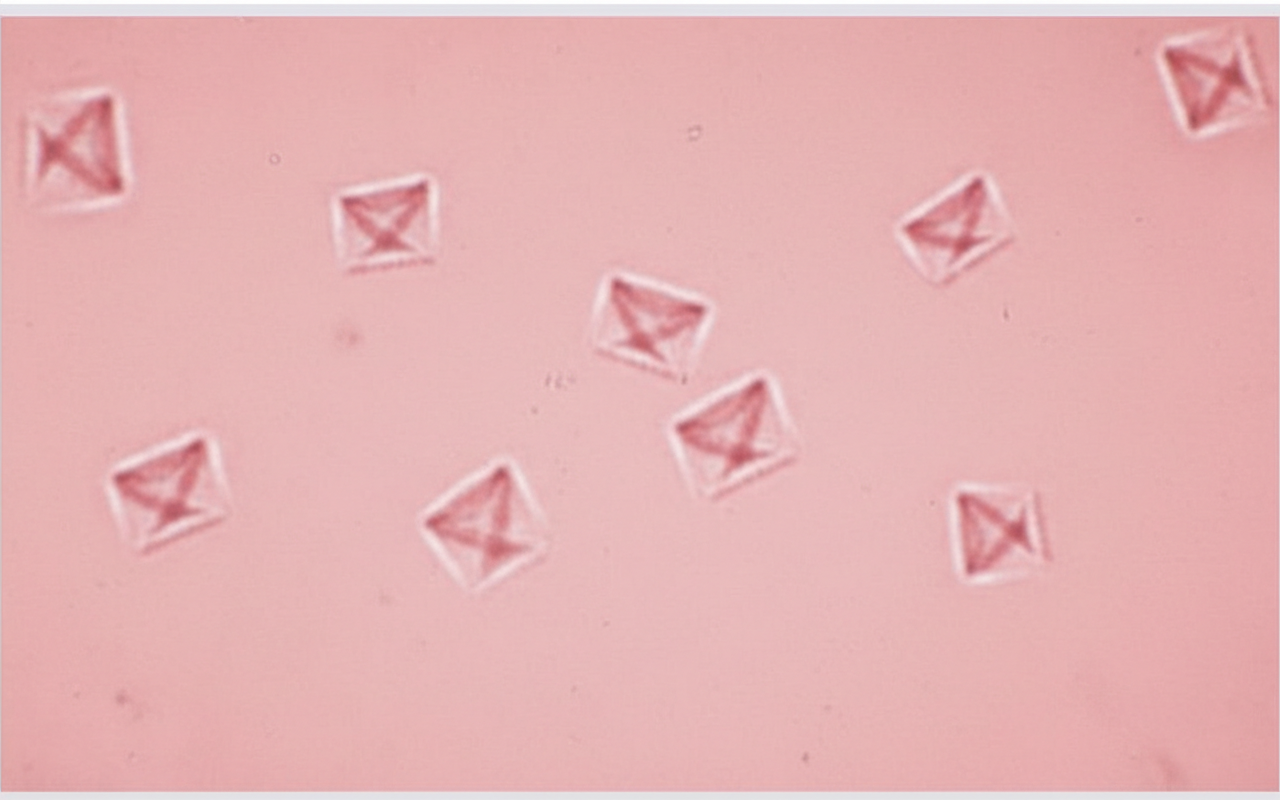
A 46-year-old man comes to the emergency department because of sharp pain in his left flank that began suddenly 30 minutes ago. Physical examination shows costovertebral angle tenderness on the left side. A photomicrograph of the urine is shown. The patient is most likely to benefit from an increase of which of the following components in the urine?
A 30-year-old man who recently emigrated from Southeast Asia presents with heartburn and a bad taste in his mouth. He says the symptoms have been present for the last 6 months and are much worse at night. He describes the pain as moderate to severe, burning in character, and localized to the epigastric region. He mentions that 1 month ago, he was tested for Helicobacter pylori back in his country and completed a course of multiple antibiotics, but there has been no improvement in his symptoms. Which of the following is the most likely diagnosis in this patient?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app