
Gastroenterology — MCQs

On this page
A 32-year-old woman presents with a three-month history of difficulty swallowing. She says that it occurs with both solids and liquids with the sensation that food is getting stuck in her throat. Additionally, the patient reports that while shoveling snow this past winter, she had noticed that her hands would lose their color and become numb. She denies any cough, regurgitation, joint pains, shortness of breath, fever, or changes in weight. She does not smoke or drink alcohol. The patient’s physical exam is within normal limits, although she does appear to have thickened, tight skin on her fingers. She does not have any other skin findings. Which antibody will most likely be found on serological study in this patient?
A 65-year-old man with chronic myelogenous leukemia comes to the physician because of severe pain and swelling in both knees for the past day. He finished a cycle of chemotherapy 1 week ago. His temperature is 37.4°C (99.4°F). Physical examination shows swelling and erythema of both knees and the base of his left big toe. Laboratory studies show: Leukocyte count 13,000/mm3 Serum Creatinine 2.2 mg/dL Calcium 8.2 mg/dL Phosphorus 7.2 mg/dL Arthrocentesis of the involved joints is most likely to show which of the following?
A 30-year-old forest landscape specialist is brought to the emergency department with hematemesis and confusion. One week ago she was diagnosed with influenza when she had fevers, severe headaches, myalgias, hip and shoulder pain, and a maculopapular rash. After a day of relative remission, she developed abdominal pain, vomiting, and diarrhea. A single episode of hematemesis occurred prior to admission. Two weeks ago she visited rainforests and caves in western Africa where she had direct contact with animals, including apes. She has no history of serious illnesses or use of medications. She is restless. Her temperature is 38.0℃ (100.4℉); the pulse is 95/min, the respiratory rate is 20/min; and supine and upright blood pressure is 130/70 mm Hg and 100/65 mm Hg, respectively. Conjunctival suffusion is noted. Ecchymoses are observed on the lower extremities. She is bleeding from one of her intravenous lines. The peripheral blood smear is negative for organisms. Filovirus genomes were detected during a reverse transcription-polymerase chain reaction. The laboratory studies show the following: Laboratory test Hemoglobin 10 g/dL Leukocyte count 1,000/mm3 Segmented neutrophils 65% Lymphocytes 20% Platelet count 50,000/mm3 Partial thromboplastin time (activated) 60 seconds Prothrombin time 25 seconds Fibrin split products positive Serum Alanine aminotransferase (ALT) 85 U/L Aspartate aminotransferase (AST) 120 U/L γ-Glutamyltransferase (GGT) 83 U/L Creatinine 2 mg/dL Which of the following is the most appropriate immediate step in management?
A 37-year-old woman comes to the physician because of difficulty swallowing for the past 1 year. She was diagnosed with gastroesophageal reflux 3 years ago and takes pantoprazole. She has smoked a pack of cigarettes daily for 14 years. Examination shows hardening of the skin of the fingers and several white papules on the fingertips. There are small dilated blood vessels on the face. Which of the following is the most likely cause of this patient's difficulty swallowing?
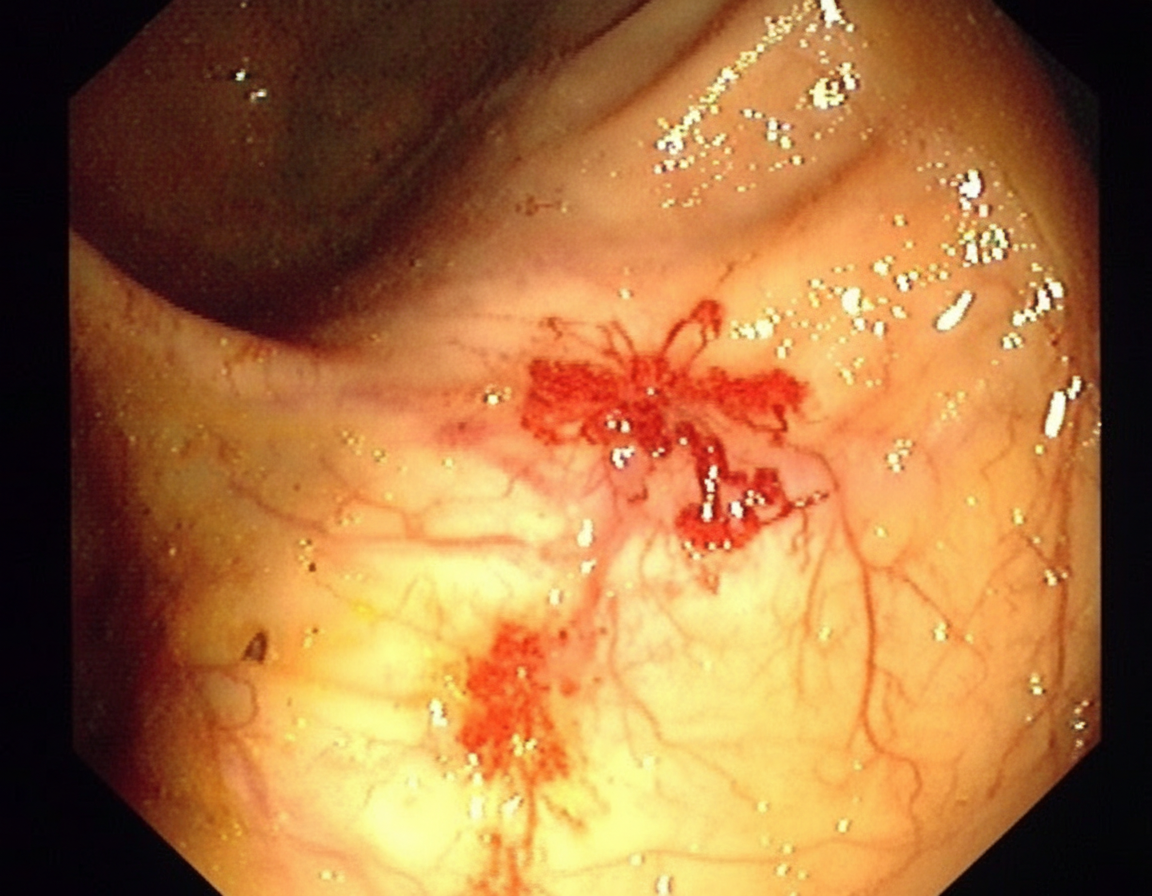
A 70-year-old man comes to the clinic for generalized fatigue. He says that he is more tired than before and has difficulty catching his breath while walking upstairs. He feels tired quickly doing his usual activity such as gardening and shopping. He does not have any symptoms of fever, change in bowel habits, abdominal pain, rectal bleeding, or weight loss. His appetite is normal. His last colonoscopy was done 10 years ago and it was normal. His blood pressure is 116/74 and heart rate is 87/min. On physical examination, his conjunctivae are pale. A routine blood test shows iron deficiency anemia with hemoglobin of 10 gm/dL. His stool is positive for occult blood. He is then sent for a colonoscopy (image is shown). What is the most likely diagnosis for the above condition?
A 63-year-old woman presents to the primary care physician’s clinic complaining of fatigue, diarrhea, headaches, and a loss of appetite. She denies any personal history of blood clots in her past, but she says that her mother has also had to be treated for pulmonary embolism in the recent past. Her past medical history is significant for preeclampsia, hypertension, polycystic ovarian syndrome, and hypercholesterolemia. She currently smokes 1 pack of cigarettes per day, drinks a glass of wine per day, and she currently denies any illicit drug use, although she has a remote past of injection drug use with heroin. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 111/min and irregular, and respiratory rate 17/min. On physical examination, her pulses are bounding and complexion is pale, but breath sounds remain clear. Oxygen saturation was initially 91% on room air and electrocardiogram (ECG) showed atrial fibrillation. Upon further discussion with the patient, her physician discovers that she is having some cognitive difficulty. The laboratory results reveal: mean corpuscular volume (MCV) 111 fL; hemoglobin (Hgb) 9.3 g/dL; methylmalonic acid (MMA) and homocysteine are both elevated. Schilling test is positive. What is the next best step in the management of this patient?
A 52-year-old woman presents with fatigue, difficulty swallowing solid foods, and frequent choking spells. She says her symptoms gradually onset 3 months ago and have progressively worsened. Past medical history is unremarkable. She reports drinking alcohol occasionally but denies smoking or illicit drug use. Her vital signs include: temperature 36.6°C (97.8°F), blood pressure 115/72 mm Hg, pulse 82/min. Physical examination shows conjunctival pallor but is otherwise unremarkable. Laboratory results are significant for the following: Hemoglobin 9.8 g/dL Red cell count 2.5 million/mm3 Mean corpuscular volume 73 μm3 Serum ferritin 9.7 ng/mL A barium swallow study is performed, which shows a proximal esophageal web. Which of the following is the most likely diagnosis in this patient?
A 57-year-old woman comes to the physician because of a 2-week history of worsening epigastric pain that improves with meals. She has had similar pain of lesser intensity for the past 4 years. Physical examination shows no abnormalities. Upper endoscopy shows a 0.5-cm mucosal breach in the anterior duodenal bulb that extends into the submucosa. A biopsy specimen of the lesion shows hypertrophy of the Brunner glands. This patient is at the greatest risk for which of the following complications?
A 23-year-old man presents to his primary care physician with complaints of fatigue and cheek pain that started a day ago. He notes that he has nasal discharge that is yellow/green as well. Otherwise, he feels well and is generally healthy. The patient has a past medical history of type I diabetes mellitus and occasionally uses IV drugs. His temperature is 99.0°F (37.2°C), blood pressure is 120/84 mmHg, pulse is 70/min, respirations are 16/min, and oxygen saturation is 98% on room air. There is pain to palpation of the left and right maxilla. Pain is worsened when the patient bends over. Which of the following is the most appropriate initial step in management?
A 42-year-old man presents to his primary care provider for abdominal pain. He reports that for several months he has been experiencing a stabbing pain above the umbilicus during meals. He denies associated symptoms of nausea, vomiting, or diarrhea. The patient’s past medical history is significant for hypertension and hyperlipidemia for which he takes amlodipine and atorvastatin. His family history is significant for lung cancer in his father. The patient is a current smoker with a 20 pack-year smoking history and drinks 3-5 beers per week. Initial laboratory testing is as follows: Serum: Na+: 141 mEq/L K+: 4.6 mEq/L Cl-: 102 mEq/L HCO3-: 25 mEq/L Urea nitrogen: 14 mg/dL Creatinine: 1.1 mg/dL Glucose: 120 mg/dL Calcium: 8.4 mg/dL Alkaline phosphatase: 66 U/L Aspartate aminotransferase (AST): 40 U/L Alanine aminotransferase (ALT): 52 U/L Gastrin: 96 pg/mL (<100 pg/mL) Lipase: 90 U/L (<160 U/L) The patient is started on a proton pump inhibitor without symptomatic improvement after 6 weeks. He is referred for an upper endoscopy, which demonstrates erosive gastritis, three ulcers in the duodenum, and one ulcer in the jejunum. Biopsy of the gastric mucosa is negative for H. pylori. Which of the following is the best next step in management?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app