
Gastroenterology — MCQs

On this page
A 68-year-old woman is brought to the emergency department with intense abdominal pain for the past 2 hours. She has had 1 episode of bloody diarrhea recently. She has an 18-year history of diabetes mellitus. She was diagnosed with hypertension and ischemic heart disease 6 years ago. She is fully alert and oriented. Her temperature is 37.5°C (99.5°F), blood pressure is 145/90 mm Hg, pulse is 78/min, and respirations are 14/min. Abdominal examination shows mild generalized abdominal tenderness without guarding or rebound tenderness. An abdominal plain X-ray shows no abnormalities. Abdominal CT reveals colonic wall thickening and pericolonic fat stranding in the splenic curvature. Bowel rest, intravenous hydration, and IV antibiotics are initiated. Which of the following is the most important diagnostic evaluation at this time?
A 27-year-old new patient presents to the physician’s office with complaints of burning, upper abdominal pain for the past 6 months. The pain does not radiate and is only partially relieved by eating small meals, over the counter antacids, and PPI. He previously underwent upper endoscopy that revealed small ulcers in the stomach and duodenum. He had to relocate across the country before he could receive proper treatment or further workup. He also complains of constipation and urinary frequency. His mother has a history of peptic ulcer disease and recurrent kidney stones. Vital signs are normal. On physical examination, the patient is alert and not under distress. Abdominal examination reveals epigastric tenderness with no rebounding. Cardiopulmonary examination is unremarkable. A fecal occult blood test is positive. Laboratory results are as follows: Sodium 142 mEq/L Potassium 4.1 mEq/L Chloride 108 mEq/L Bicarbonate 22 mEq/L Calcium 11.2 mg/dL Phosphorus 2.0 mg/dL Blood urea nitrogen 19 mg/dL Creatinine 1.1 mg/dL Additional evaluation is most likely to reveal which of the following?
A 53-year-old patient presents to his primary care provider with a 1-week history of abdominal pain at night and between meals. He has attempted taking antacids, which help briefly, but then the pain returns. The patient has not noticed any changes to the color of his stool but states that he has been having some loose bowel movements. The patient reports that he has had duodenal ulcers in the past and is concerned that this is a recurrence. On exam, his temperature is 98.4°F (36.9°C), blood pressure is 130/84 mmHg, pulse is 64/min, and respirations are 12/min. The abdomen is soft, nontender, and nondistended in clinic today. A fecal occult blood test is positive for blood in the stool. During outpatient workup, H. pylori stool antigen is negative, endoscopy demonstrates duodenal ulcers, and gastrin levels are elevated after a secretin stimulation test. Which of the following should also be examined in this patient?
A 33-year-old woman comes to the clinic for a follow-up visit after recently starting high dose corticosteroids for a newly diagnosed autoimmune condition. She was first evaluated a month ago due to fatigue, muscle weakness, and a scaly rash on both hands. On examination, muscle strength was rated 2 out of 5 in the upper extremities. Creatine kinase-MB was elevated, and anti-Jo-1 antibodies were observed. A muscle biopsy later showed perimysial inflammation and treatment was initiated. Today, the patient says that her symptoms have not improved despite treatment with corticosteroids. It is agreed upon to initiate methotrexate with the hopes of achieving better symptom control. Which of the following is most often associated with this patient’s condition?
A 45-year-old woman presents to the clinic with a variety of complaints on different areas of her body, including telangiectasias on both the upper and lower extremities, bluish discoloration of the fingertips when exposed to cold, and burning midsternal chest pain. She is a tobacco smoker and works as a school teacher. After evaluation, an anti-centromere antibody test is ordered, and returns with an elevated titer. Which of the following symptoms are least likely to be seen in this patient's condition?
A 25-year-old man presents to the emergency department after numerous episodes of vomiting. The patient states that he thinks he ‘ate something weird’ and has been vomiting for the past 48 hours. He says that he came to the hospital because the last few times he "threw up blood". He is hypotensive with a blood pressure of 90/55 mm Hg and a pulse of 120/min. After opening an intravenous line, a physical examination is performed which is normal except for mild epigastric tenderness. An immediate endoscopy is performed and a tear involving the mucosa and submucosa of the gastroesophageal junction is visualized. Which of the following is the most likely diagnosis?
A 55-year-old man presents to his primary care physician for trouble swallowing. The patient claims that he used to struggle when eating food if he did not chew it thoroughly, but now he occasionally struggles with liquids as well. He also complains of a retrosternal burning sensation whenever he eats. He also claims that he feels his throat burns when he lays down or goes to bed. Otherwise, the patient has no other complaints. The patient has a past medical history of obesity, diabetes, constipation, and anxiety. His current medications include insulin, metformin, and lisinopril. On review of systems, the patient endorses a 5 pound weight loss recently. The patient has a 22 pack-year smoking history and drinks alcohol with dinner. His temperature is 99.5°F (37.5°C), blood pressure is 177/98 mmHg, pulse is 90/min, respirations are 17/min, and oxygen saturation is 98% on room air. On physical exam, you note an overweight man in no current distress. Abdominal exam is within normal limits. Which of the following is the best next step in management?
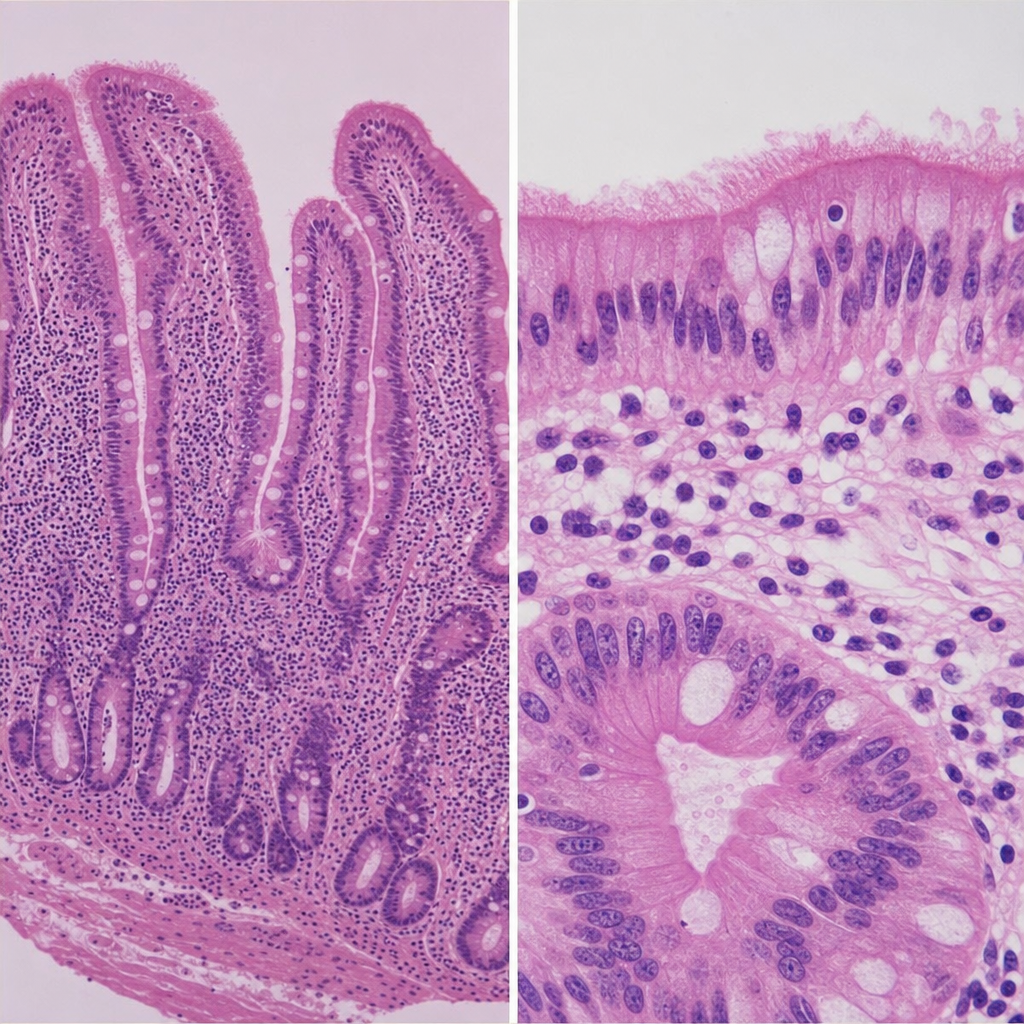
A 34-year-old man comes to the physician because of foul-smelling diarrhea, fatigue, and bloating for 6 months. During this time, he has had a 5-kg (11-lb) weight loss without a change in diet. He has type 1 diabetes mellitus that is well-controlled with insulin. Examination shows conjunctival pallor and inflammation of the corners of the mouth. The abdomen is soft, and there is diffuse tenderness to palpation with no guarding or rebound. His hemoglobin concentration is 10.4 g/dL. The patient undergoes upper endoscopy. A photomicrograph of tissue from an intestinal biopsy is shown. Which of the following is most likely to improve this patient's symptoms?
A 33-year-old HIV-positive male is seen in clinic for follow-up care. When asked if he has been adhering to his HIV medications, the patient exclaims that he has been depressed, thus causing him to not take his medication for six months. His CD4+ count is now 33 cells/mm3. What medication(s) should he take in addition to his anti-retroviral therapy?
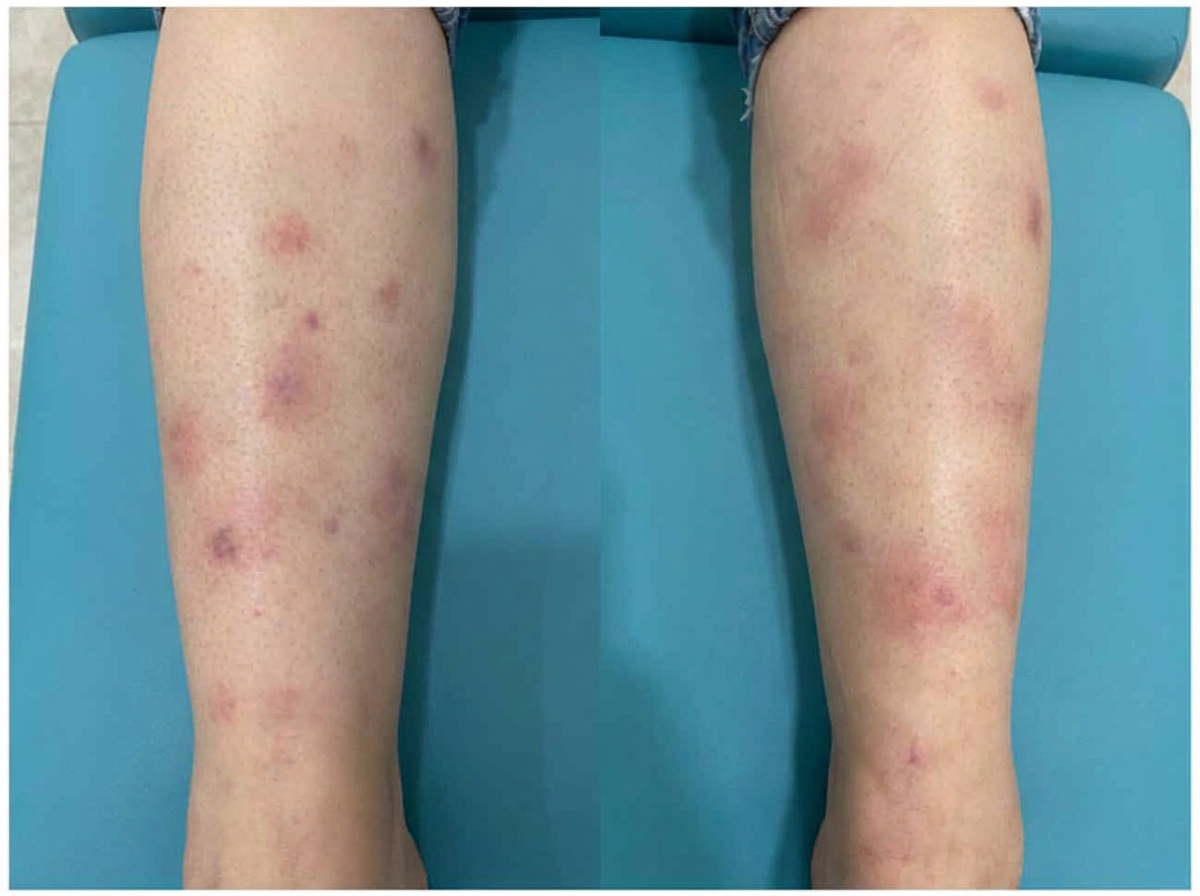
A 42-year-old man presents to the physician with a painful ulcer in the mouth for 1 week. He has had similar episodes of ulcers over the past year. Every episode lasts about a week and heals without leaving a scar. He has also had similar ulcers on the scrotum, but the ulcers have left scars. He takes no medications. His temperature is 36.8°C (98.2°F), and the rest of the vital signs are stable. On physical examination, a 1-cm yellowish ulcer with a necrotic base is seen on the right buccal mucosa. Also, there are several tender nodules of different sizes on both shins. An image of one of the nodules is shown. Which of the following is the most likely complication of this patient’s current condition?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app