
GI bleeding (upper and lower) — MCQs

A 22-year-old woman comes to the emergency department because of chest and epigastric pain that started just after vomiting 30 minutes ago. She does not take any medications and does not drink alcohol or smoke cigarettes. While in the emergency department, the patient experiences two episodes of forceful, bloody emesis. Her temperature is 99.1°F (37.3°C), pulse is 110/minute, and blood pressure is 105/60 mm Hg. Physical examination shows dental enamel erosion and calluses on the dorsal aspect of her right hand. There is tenderness to palpation in the epigastrium. An x-ray of the chest is normal. Further evaluation of this patient is most likely to show which of the following findings?
A 14-month-old boy has iron-deficiency anemia refractory to iron therapy. His stool is repeatedly positive for occult blood. The parents bring the child to the emergency room after they notice some blood in his stool. Which of the following is the diagnostic gold standard for this patient's most likely condition?
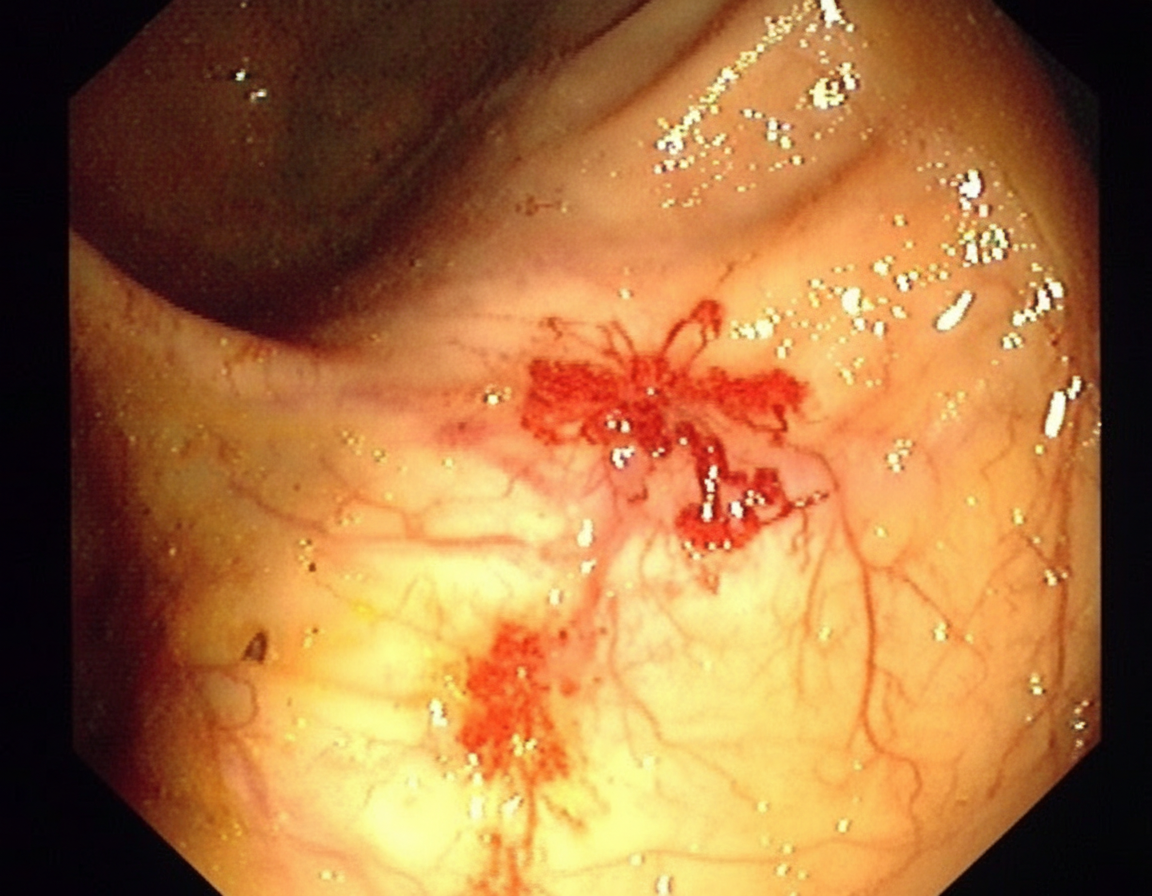
A 70-year-old man comes to the clinic for generalized fatigue. He says that he is more tired than before and has difficulty catching his breath while walking upstairs. He feels tired quickly doing his usual activity such as gardening and shopping. He does not have any symptoms of fever, change in bowel habits, abdominal pain, rectal bleeding, or weight loss. His appetite is normal. His last colonoscopy was done 10 years ago and it was normal. His blood pressure is 116/74 and heart rate is 87/min. On physical examination, his conjunctivae are pale. A routine blood test shows iron deficiency anemia with hemoglobin of 10 gm/dL. His stool is positive for occult blood. He is then sent for a colonoscopy (image is shown). What is the most likely diagnosis for the above condition?
A 57-year-old man is brought to the emergency department by his family because of several episodes of vomiting of blood in the past 24 hours. He has a history of alcoholic cirrhosis and is being treated for ascites with diuretics and for encephalopathy with lactulose. His vital signs include a temperature of 36.9°C (98.4°F), pulse of 85/min, and blood pressure of 80/52 mm Hg. On examination, he is confused and unable to give a complete history. He is noted to have jaundice, splenomegaly, and multiple spider angiomas over his chest. Which of the following is the best initial management of this patient?
A 25-year-old man presents to the emergency department after numerous episodes of vomiting. The patient states that he thinks he ‘ate something weird’ and has been vomiting for the past 48 hours. He says that he came to the hospital because the last few times he "threw up blood". He is hypotensive with a blood pressure of 90/55 mm Hg and a pulse of 120/min. After opening an intravenous line, a physical examination is performed which is normal except for mild epigastric tenderness. An immediate endoscopy is performed and a tear involving the mucosa and submucosa of the gastroesophageal junction is visualized. Which of the following is the most likely diagnosis?
A 65-year-old patient presents with acute left lower quadrant abdominal pain and is diagnosed with diverticulitis. Which of the following is most likely to have prevented this patient's condition?
A 41-year-old male presents to his primary care provider after seeing bright red blood in the toilet bowl after his last two bowel movements. He reports that the second time he also noticed some blood mixed with his stool. The patient denies abdominal pain and any changes in his stool habits. He notes a weight loss of eight pounds in the last two months. His past medical history is significant for an episode of pancreatitis two years ago for which he was hospitalized for several days. He drinks 2-3 beers on the weekend, and he has never smoked. He has no family history of colon cancer. His temperature is 97.6°F (36.4°C), blood pressure is 135/78 mmHg, pulse is 88/min, and respirations are 14/min. On physical exam, his abdomen is soft and nontender to palpation. Bowel sounds are present, and there is no hepatomegaly. Which of the following is the best next step in diagnosis?
A 74-year-old man is brought to the emergency department after he had copious amounts of blood-stained stools. Minutes later, he turned sweaty, felt light-headed, and collapsed into his wife’s arms. Upon admission, he is found to have a blood pressure of 78/40 mm Hg, a pulse of 140/min, and oxygen saturation of 98%. His family history is relevant for both gastric and colorectal cancer. His personal history is relevant for hypertension, for which he takes amlodipine. After an initial successful resuscitation with intravenous fluids, which of the following should be the first step in approaching this case?
A 68-year-old woman presents to her primary care physician with a complaint of fatigue, difficulty breathing upon exertion, and crampy lower abdominal pain. She also noticed that her stools appear darker than usual. She has had essential hypertension for 20 years, for which she takes bisoprolol. Her family history is positive for type 2 diabetes mellitus. On physical examination, she looks pale. Complete blood count shows the following: Hemoglobin 10 g/dL Mean corpuscular volume (MCV) 70 fL Mean corpuscular hemoglobin (MCH) 25 pg/cell Mean corpuscular hemoglobin concentration (MCHC) 27 g/dL Red cell distribution width 16% Platelet count 350,000/mm3 Serum ferritin 9 ng/mL Which of the following is the best initial step for this patient?
A 72-year-old male with a past medical history significant for aortic stenosis and hypertension presents to the emergency department complaining of weakness for the past 3 weeks. He states that, apart from feeling weaker, he also has noted lightheadedness, pallor, and blood-streaked stools. The patient's vital signs are stable, and he is in no acute distress. Laboratory workup reveals that the patient is anemic. Fecal occult blood test is positive for bleeding. EGD was performed and did not reveal upper GI bleeding. Suspecting a lower GI bleed, a colonoscopy is performed after prepping the patient, and it is unremarkable. What would be an appropriate next step for localizing a lower GI bleed in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app