
Celiac disease — MCQs

A 35-year-old Caucasian female presents with anemia, malaise, bloating, and diarrhea. Past genetic testing revealed that this patient carries the HLA-DQ2 allele. The physician suspects that the patient's presentation is dietary in cause. Which of the following findings would definitively confirm this diagnosis?
A 23-year-old man presents to the office complaining of weight loss and fatigue for the past 2 months. He states that he has been experiencing foul-smelling, light-colored stools but thinks it is because he hasn’t been eating well, recently. He has a past medical history significant for cystic fibrosis, which is well-controlled medically. He denies any shortness of breath, chest or abdominal pain, nausea, vomiting, or melena. On physical examination, his skin is pale and dry. Which of the following would be the most likely etiology of a malabsorption syndrome giving rise to this patient’s current condition?
A previously healthy 20-year-old woman comes to the physician because of recurrent abdominal cramps, bloating, and diarrhea for 4 months. She describes her stools as greasy, foul-smelling, and difficult to flush. During this time she has had a 6-kg (13.2-lb) weight loss. She has no personal or family history of serious illness. Physical examination shows pallor and cheilitis. Laboratory studies show a hemoglobin concentration of 11 g/dL. Serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference range. Test of the stool for occult blood is negative and stool microscopy reveals no pathogens and no leukocytes. Analysis of a 24-hour stool sample shows 12 g of fat. The patient is asked to consume 25 g of d-xylose. Five hours later, its concentration is measured in urine at 2 g (N = > 4 g/5 h). The test is repeated after a two-week course of rifaximin, but the urinary concentration of d-xylose remains the same. Which of the following is the most likely diagnosis?
An 82-year-old woman presents with 2 months of foul-smelling, greasy diarrhea. She says that she also has felt very tired recently and has had some associated bloating and flatus. She denies any recent abdominal pain, nausea, melena, hematochezia, or vomiting. She also denies any history of recent travel and states that her home has city water. Which of the following tests would be most appropriate to initially work up the most likely diagnosis in this patient?
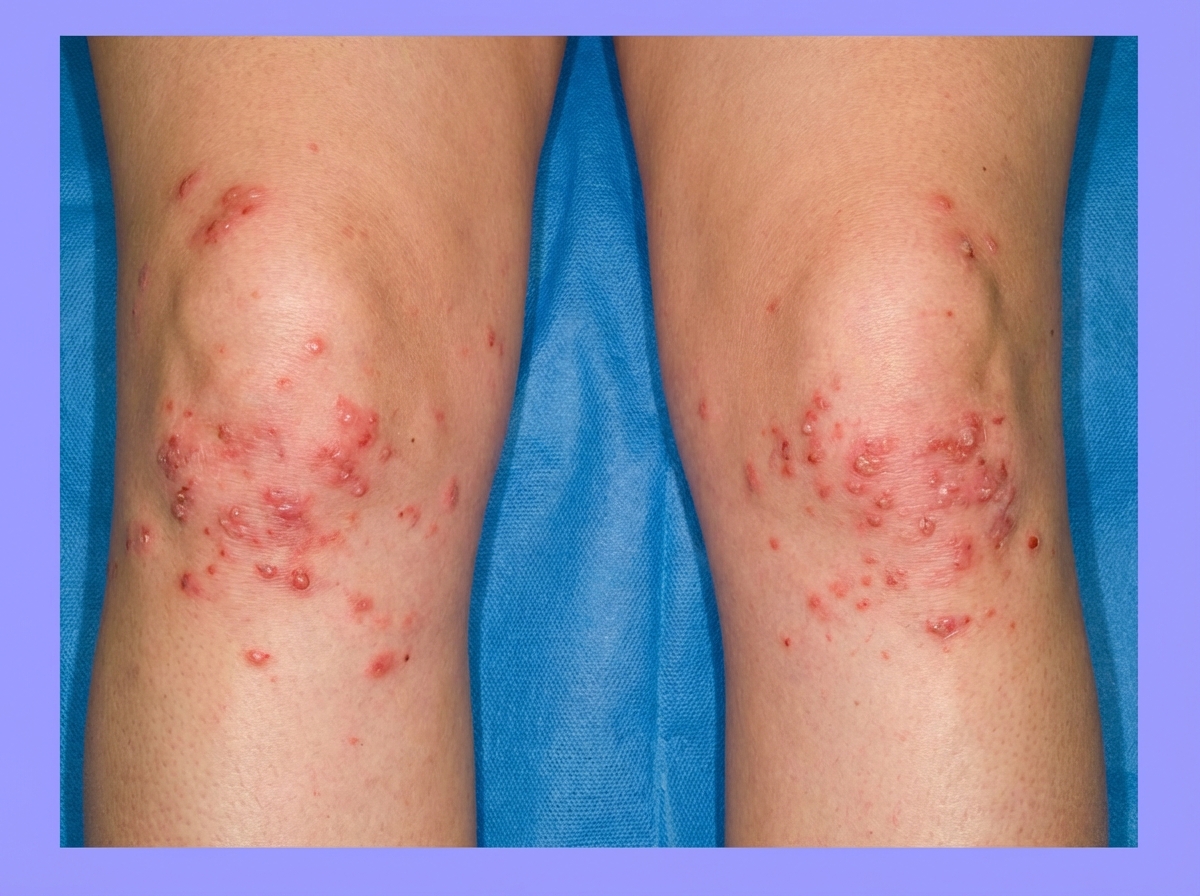
A 24-year-old man comes to the physician for the evaluation of a severely pruritic skin rash. Physical examination shows a symmetrical rash over the knees and elbows with tense, grouped vesicles, and several excoriation marks. Microabscesses in the papillary dermis are seen on light microscopy. Immunofluorescence shows deposits of immunoglobulin A at the tips of dermal papillae. This patient's skin findings are most likely associated with which of the following?
A 24-year-old woman with 45,X syndrome comes to the physician because of diarrhea for 4 months. She also reports bloating, nausea, and abdominal discomfort that persists after defecation. For the past 6 months, she has felt tired and has been unable to do her normal chores. She went on a backpacking trip across Southeast Asia around 7 months ago. She is 144 cm (4 ft 9 in) tall and weighs 40 kg (88 lb); BMI is 19 kg/m2. Her blood pressure is 110/60 mm Hg in the upper extremities and 80/40 mm Hg in the lower extremities. Examination shows pale conjunctivae and angular stomatitis. Abdominal examination is normal. Laboratory studies show: Hemoglobin 9.1 mg/dL Leukocyte count 5100/mm3 Platelet count 200,000/mm3 Mean corpuscular volume 67 μmm3 Serum Na+ 136 mEq/L K+ 3.7 mEq/L Cl- 105 mEq/L Glucose 89 mg/dL Creatinine 1.4 mg/dL Ferritin 10 ng/mL IgA tissue transglutaminase antibody positive Based on the laboratory studies, a biopsy for confirmation of the diagnosis is suggested, but the patient is unwilling to undergo the procedure. Which of the following is the most appropriate next step in management of this patient's gastrointestinal symptoms?
A 54-year-old man comes to the physician because of diarrhea that has become progressively worse over the past 4 months. He currently has 4–6 episodes of foul-smelling stools per day. Over the past 3 months, he has had fatigue and a 5-kg (11-lb) weight loss. He returned from Bangladesh 6 months ago after a year-long business assignment. He has osteoarthritis and hypertension. Current medications include amlodipine and naproxen. He appears pale and malnourished. His temperature is 37.3°C (99.1°F), pulse is 76/min, and blood pressure is 140/86 mm Hg. Examination shows pale conjunctivae and dry mucous membranes. Angular stomatitis and glossitis are present. The abdomen is distended but soft and nontender. Rectal examination shows no abnormalities. Laboratory studies show: Hemoglobin 8.9 g/dL Leukocyte count 4100/mm3 Platelet count 160,000/mm3 Mean corpuscular volume 110 μm3 Serum Na+ 133 mEq/L Cl- 98 mEq/l K+ 3.3 mEq/L Creatinine 1.1 mg/dL IgA 250 mg/dL Anti-tissue transglutaminase, IgA negative Stool culture and studies for ova and parasites are negative. Test of the stool for occult blood is negative. Fecal fat content is 22 g/day (N < 7). Fecal lactoferrin is negative and elastase is within normal limits. Which of the following is the most appropriate next step in diagnosis?
A 42-year-old woman presents with exertional dyspnea and fatigue for the past 3 months. Her past medical history is significant for multiple episodes of mild diarrhea for many years, which was earlier diagnosed as irritable bowel syndrome (IBS). She denies any current significant gastrointestinal symptoms. The patient is afebrile and vital signs are within normal limits. Physical examination reveals oral aphthous ulcers and mild conjunctival pallor. Abdominal examination is unremarkable. There is a rash present on the peripheral extremities bilaterally (see image). Laboratory findings are significant for evidence of microcytic hypochromic anemia. FOBT is negative. Which of the following is the most likely diagnosis in this patient?
A 74-year-old woman presents to the clinic for evaluation of an erythematous and edematous skin rash on her right leg that has progressively worsened over the last 2 weeks. The medical history is significant for hypertension and diabetes mellitus type 2. She takes prescribed lisinopril and metformin. The vital signs include: blood pressure 152/92 mm Hg, heart rate 76/min, respiratory rate 12/min, and temperature 37.8°C (100.1°F). On physical exam, the patient appears alert and oriented. Observation of the lesion reveals a poorly demarcated region of erythema and edema along the anterior aspect of the right tibia. Within the region of erythema is a 2–3 millimeter linear break in the skin that does not reveal any serous or purulent discharge. Tenderness to palpation and warmth is associated with the lesion. There are no vesicles, pustules, papules, or nodules present. Ultrasound of the lower extremity is negative for deep vein thrombosis or skin abscess. The blood cultures are pending. Which of the following is the most likely diagnosis based on history and physical examination?
A 21-year-old woman presents with malaise, joint pains, and a rash that worsens with sun exposure. Examination reveals an erythematous facial rash with edema. Her complete blood count shows lymphocytopenia. In addition to the most likely diagnosis, which of the following disorders can also cause lymphocytopenia? I. HIV II. Autoimmune disorders III. Tuberculosis IV. Lymphoma V. Hypersplenism
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app