
Gastroenterology — MCQs

On this page
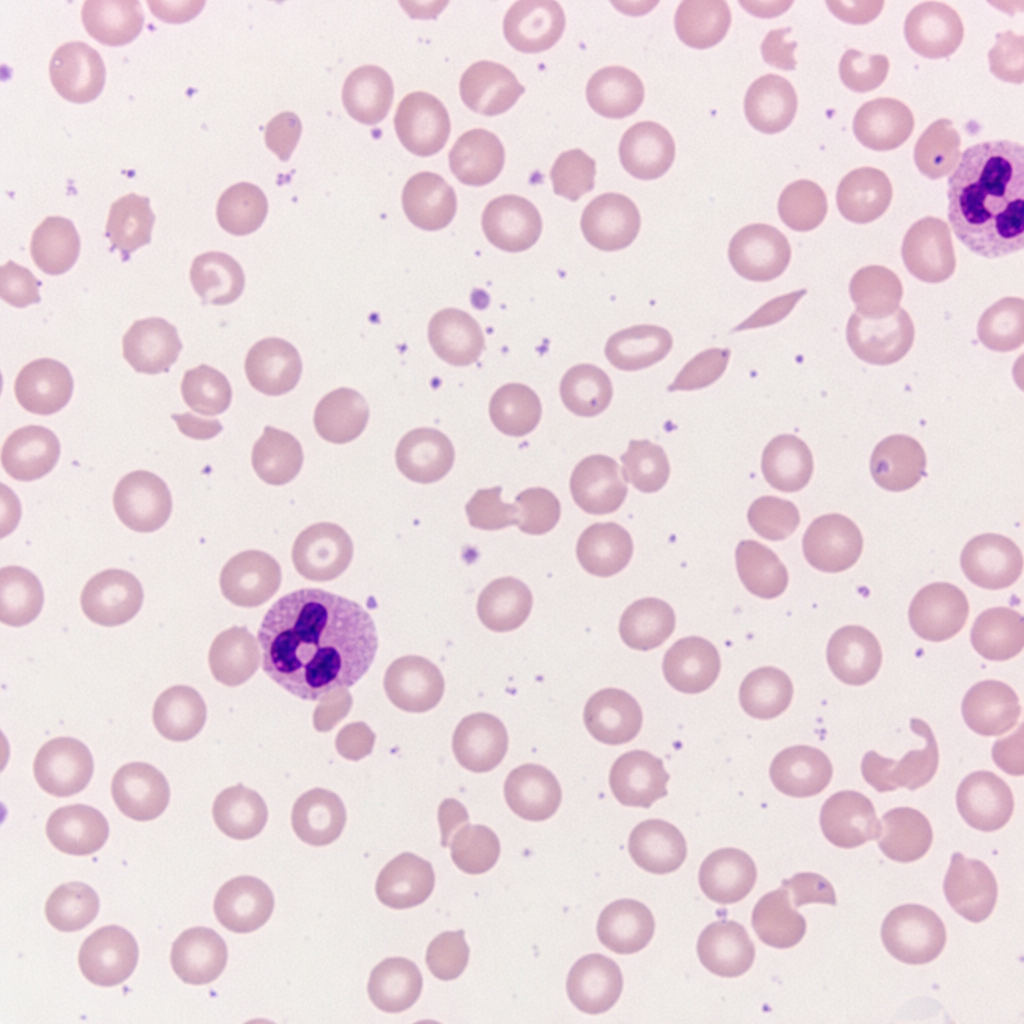
A 34-year-old woman is evaluated for a 4-month history of fatigue, pallor, and exertional dyspnea. She has a history of systemic lupus erythematosus managed with hydroxychloroquine. Laboratory results show hemoglobin 7.8 g/dL, MCV 88 fL, reticulocyte count 8.2% (corrected reticulocyte index 3.9), total bilirubin 3.4 mg/dL (indirect 2.9 mg/dL), LDH 520 U/L, and haptoglobin less than 10 mg/dL. Urinalysis reveals 1+ proteinuria with no RBC casts. Direct antiglobulin test (DAT) is positive for IgG. Which of the following is the most appropriate first-line treatment?
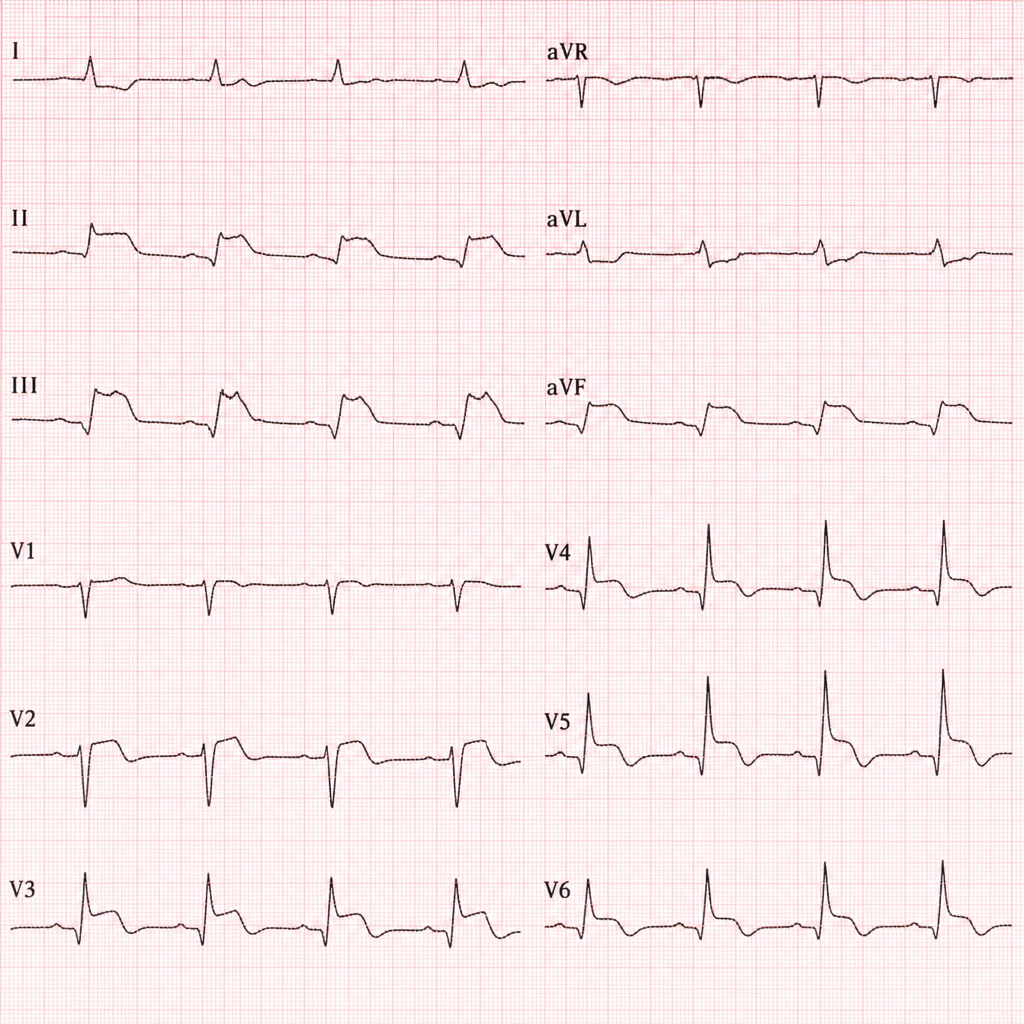
A 67-year-old woman with a history of hypertension and type 2 diabetes presents to the emergency department with 3 hours of epigastric discomfort, diaphoresis, and mild dyspnea. She denies chest pain. Her blood pressure is 148/92 mmHg, heart rate 98 bpm, respiratory rate 20/min, and oxygen saturation 94% on room air. ECG shows ST elevation in leads II, III, and aVF with reciprocal ST depression in leads I and aVL. Troponin I is 2.4 ng/mL (reference <0.04). The cath lab is available. Which of the following is the most appropriate next step in management?
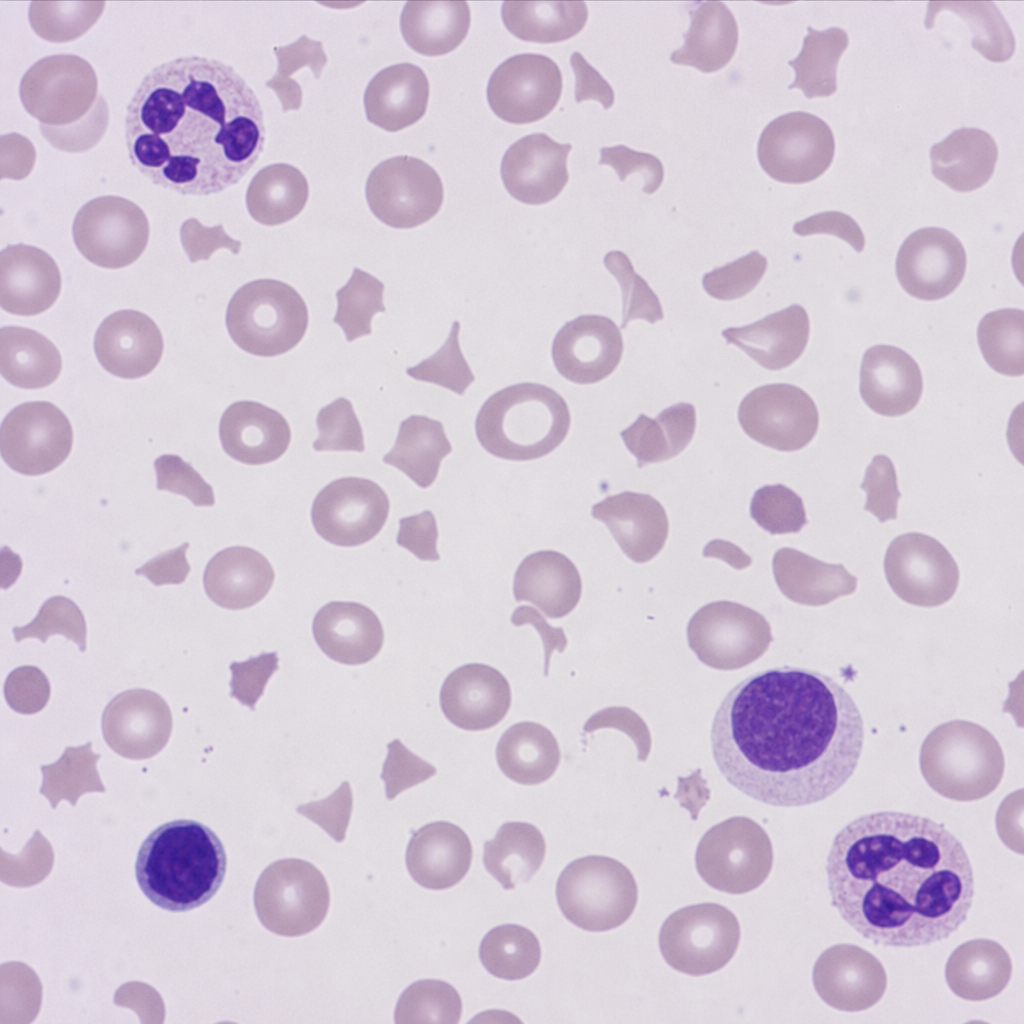
A 45-year-old woman presents with a 6-week history of fatigue, pallor, and jaundice. She has no significant past medical history and takes no medications. Laboratory results show: hemoglobin 7.2 g/dL, MCV 92 fL, reticulocyte count 8%, total bilirubin 3.8 mg/dL (indirect 3.1 mg/dL), LDH 780 U/L, haptoglobin undetectable, and platelet count 48,000/µL. A peripheral blood smear is shown above, demonstrating schistocytes and helmet cells consistent with microangiopathic hemolytic anemia. Direct antiglobulin test (DAT) is negative. Which of the following is the most likely underlying mechanism responsible for this patient's anemia?
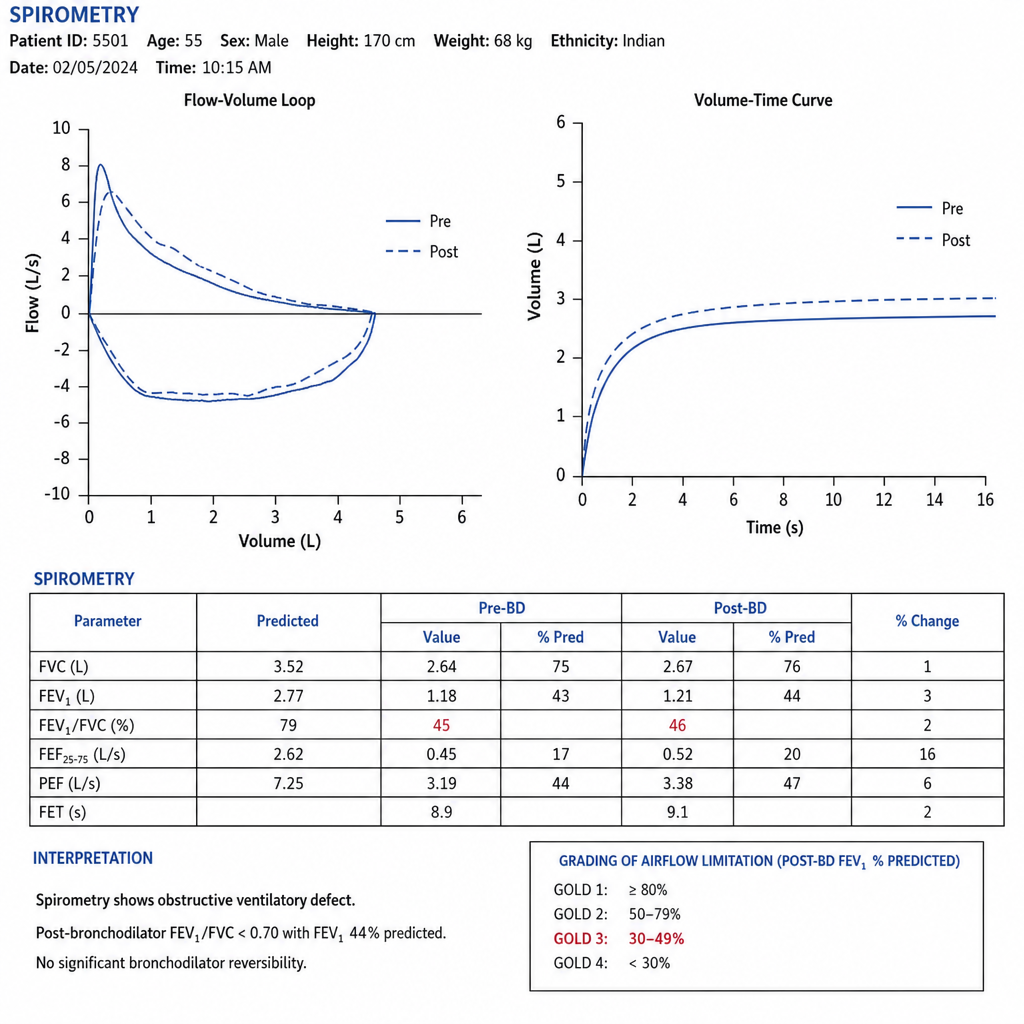
A 55-year-old man with a 30-pack-year smoking history presents with progressive dyspnea over 3 years, now limiting him to walking less than one block (mMRC grade 3; CAT score 24). He has a chronic productive cough. He is not currently on any maintenance inhaler therapy and uses only a short-acting beta-agonist as needed. Spirometry shows a post-bronchodilator FEV1/FVC of 0.58, FEV1 of 44% of predicted, and FVC of 76% of predicted, consistent with an obstructive pattern and scooped expiratory limb on the flow-volume loop. His blood eosinophil count is 320 cells/µL. He has had two exacerbations requiring oral steroids in the past year but no hospitalizations. Which of the following is the most appropriate change to his maintenance therapy?
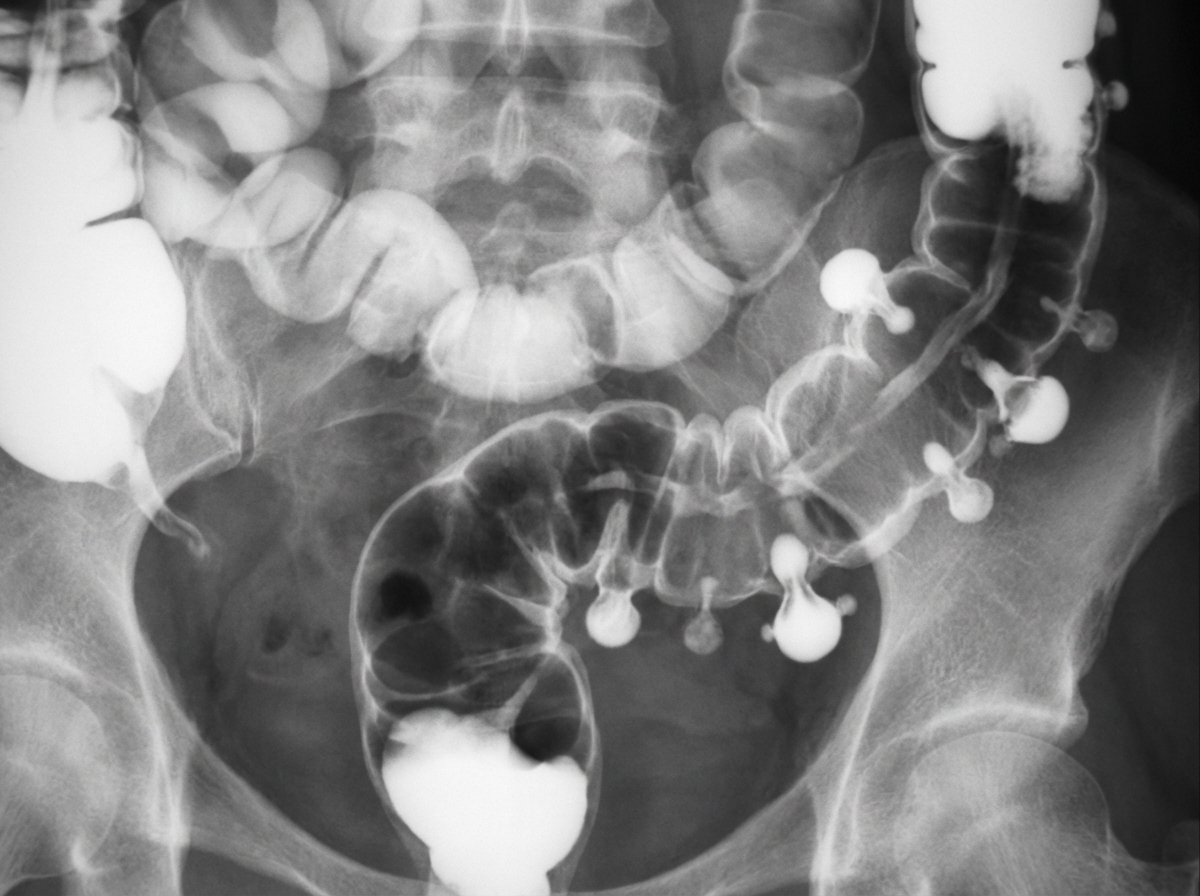
A 30-year-old patient presents with loose stools, lower abdominal pain, weight loss, diarrhea and passage of blood and mucus. On sigmoidoscopy this is the presentation of the patient. All of the following statements regarding this condition are true except:

All of the following statements regarding this picture are true except:
The following pus was drained from a liver abscess. Which complication(s) is/are seen with this condition?
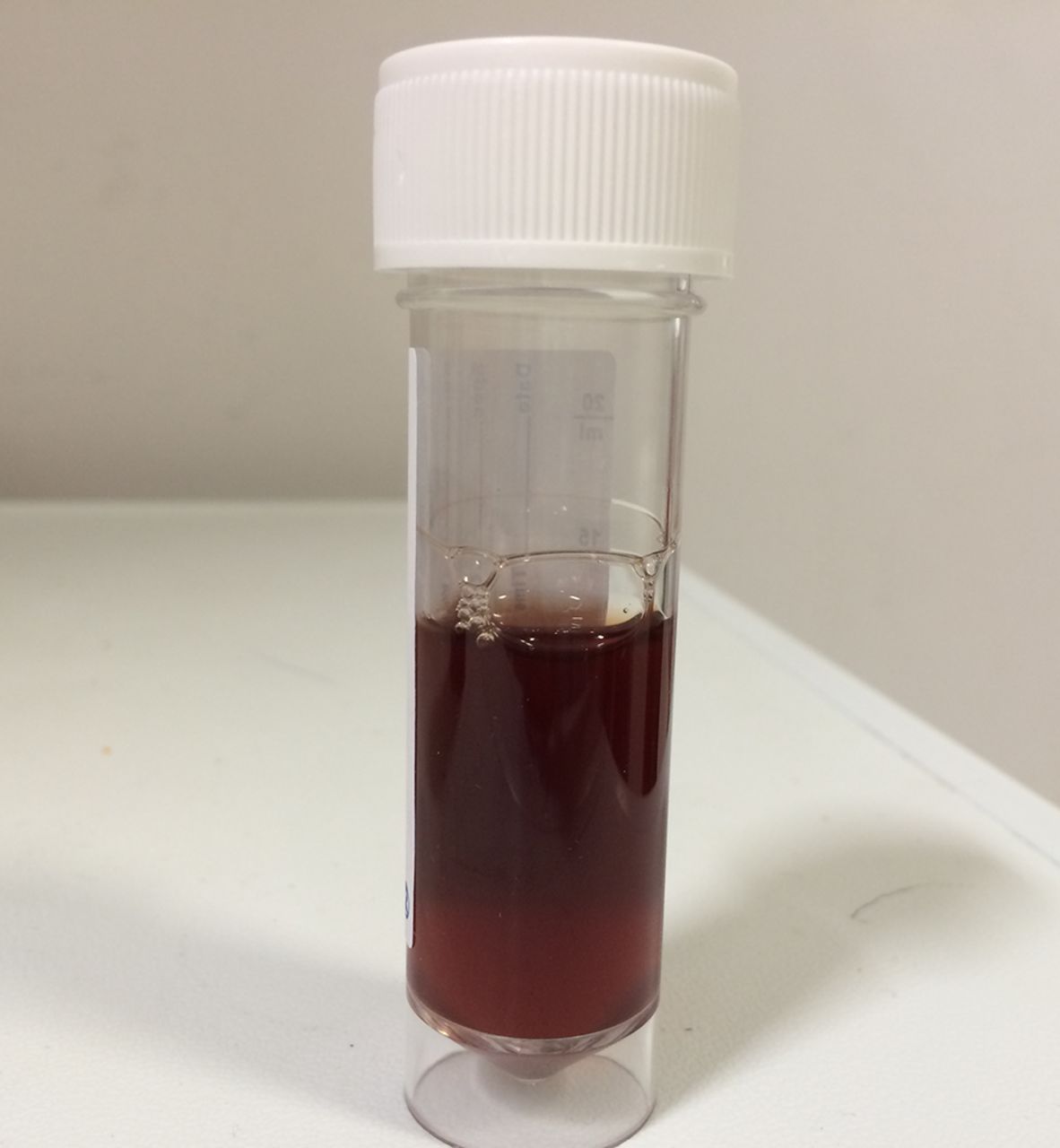
The following pus was drained from a liver abscess. Diagnosis is:

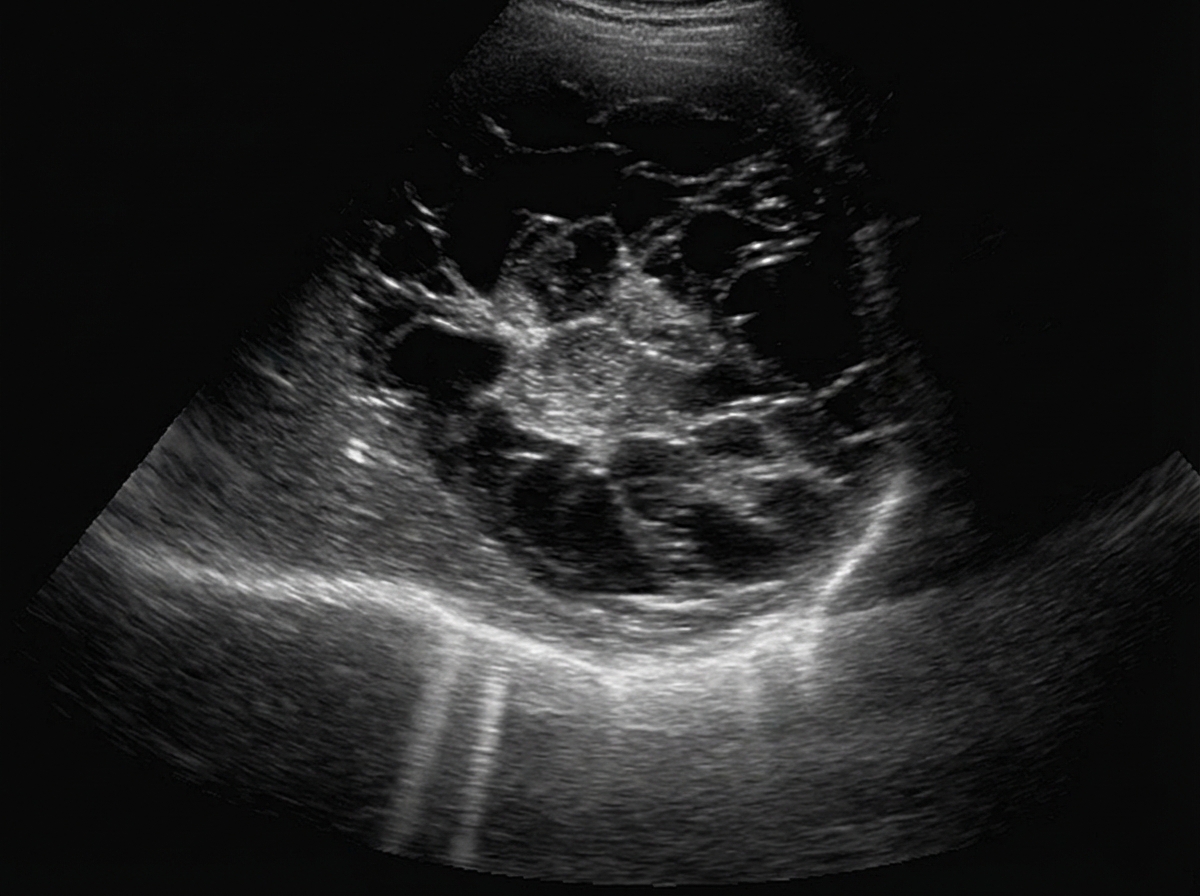
All investigations should be done in this case except:

A 25 -year-old shepherd presents with continuous discomfort in right hypochondrium and on examination shows presence of enlarged liver 8 cm below costal margins. The probable diagnosis is:
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app