
Endocrinology (diabetes, thyroid disorders) — MCQs

On this page
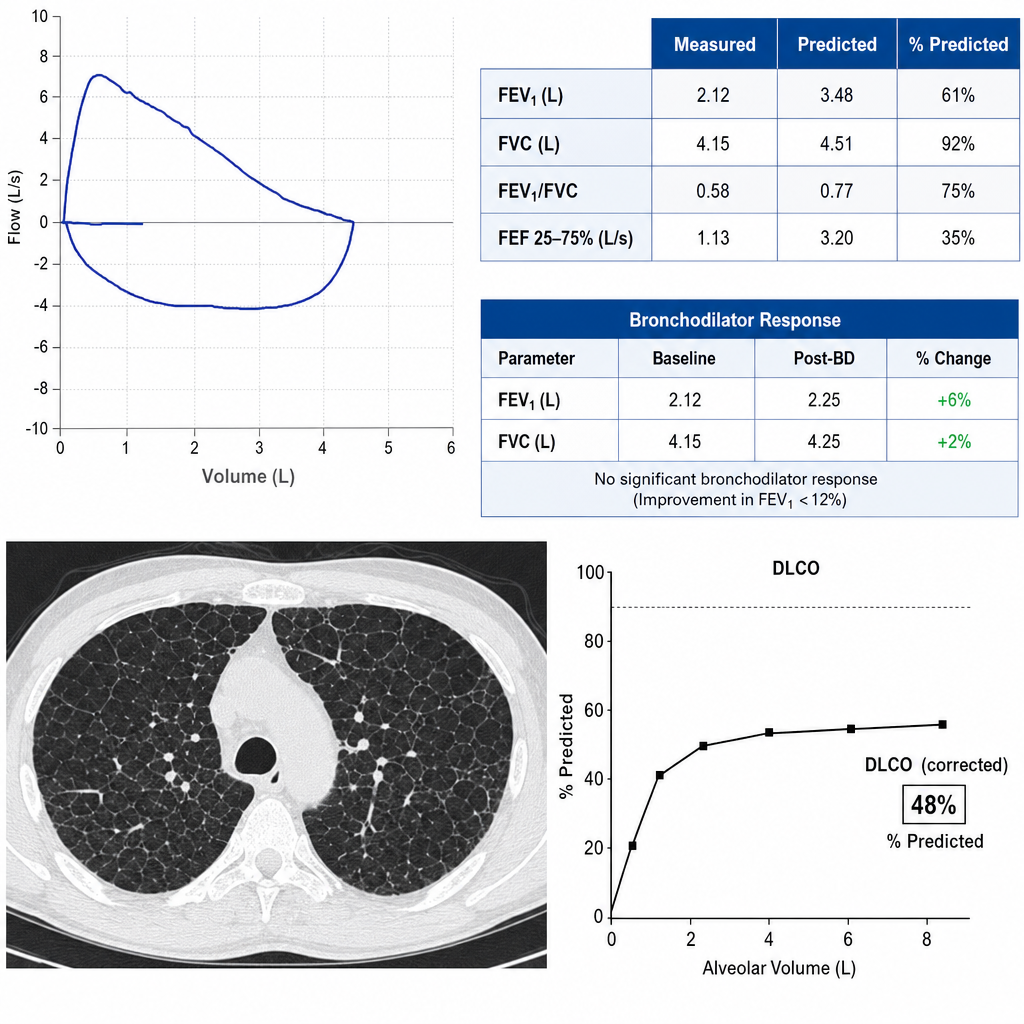
A 44-year-old man with a 20-pack-year smoking history presents with progressive exertional dyspnea over 18 months. He denies cough, fever, or weight loss. Pulmonary function testing is performed. FEV₁/FVC is 0.58, FVC is 92% of predicted, FEV₁ is 61% of predicted, and there is no significant bronchodilator response (improvement in FEV₁ <12%). DLCO is 48% of predicted. Which of the following best characterizes the physiologic pattern and its most likely underlying cause?
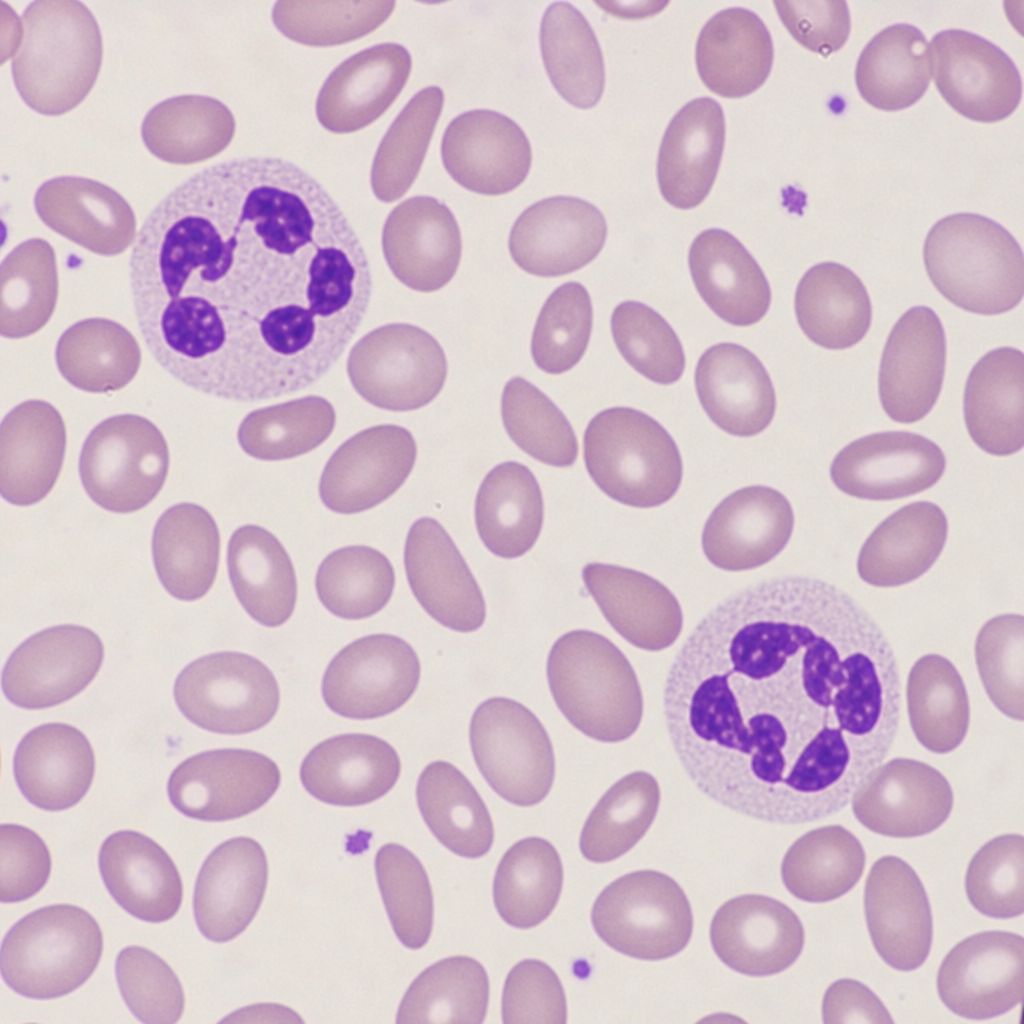
A 38-year-old woman with a 10-year history of Crohn's disease involving the terminal ileum and right colon presents with a 6-month history of fatigue, pallor, and glossitis. She underwent an ileocecal resection 2 years ago. Labs: Hgb 8.4 g/dL, MCV 108 fL, WBC 4,100/μL, platelets 140,000/μL, reticulocyte count 0.8%. Peripheral blood smear demonstrates hypersegmented neutrophils and macro-ovalocytes. Serum folate is normal. Which of the following is the most appropriate next step in management?
A 65-year-old man with newly diagnosed type 2 diabetes (HbA1c 9.5%) has established atherosclerotic cardiovascular disease (prior MI) and diabetic kidney disease (eGFR 40, albuminuria 500 mg/g). His cardiologist recommends an SGLT2 inhibitor, his nephrologist recommends a GLP-1 agonist, and the primary care physician suggests starting insulin for rapid control. Evaluate the optimal evidence-based treatment strategy.
A 48-year-old woman presents with a 3 cm thyroid nodule discovered incidentally. TSH is 2.5 mIU/L (normal). FNA biopsy shows Bethesda Category IV (follicular neoplasm). Molecular testing shows a RAS mutation. She is anxious about cancer and requests total thyroidectomy. Her surgeon suggests thyroid lobectomy. Synthesize the best management approach considering oncologic outcomes, quality of life, and patient preferences.
A 32-year-old woman with type 1 diabetes for 20 years presents with recurrent severe hypoglycemia despite optimal insulin management and continuous glucose monitoring. She has hypoglycemia unawareness and two recent episodes requiring emergency glucagon. HbA1c is 6.8%. She has gastroparesis and proliferative retinopathy but preserved kidney function (eGFR >60). Her endocrinologist is considering islet cell transplantation. Evaluate the appropriateness of this intervention.
Practice by Chapter
Type 1 diabetes mellitus
Practice Questions
Type 2 diabetes mellitus
Practice Questions
Diabetic ketoacidosis
Practice Questions
Hyperosmolar hyperglycemic state
Practice Questions
Diabetes complications and screening
Practice Questions
Insulin and oral antidiabetic agents
Practice Questions
Thyroid function testing
Practice Questions
Hypothyroidism
Practice Questions
Hyperthyroidism and thyroiditis
Practice Questions
Thyroid nodules and cancer
Practice Questions
Adrenal disorders
Practice Questions
Pituitary disorders
Practice Questions
Metabolic bone disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app