
Supraventricular tachycardias — MCQs

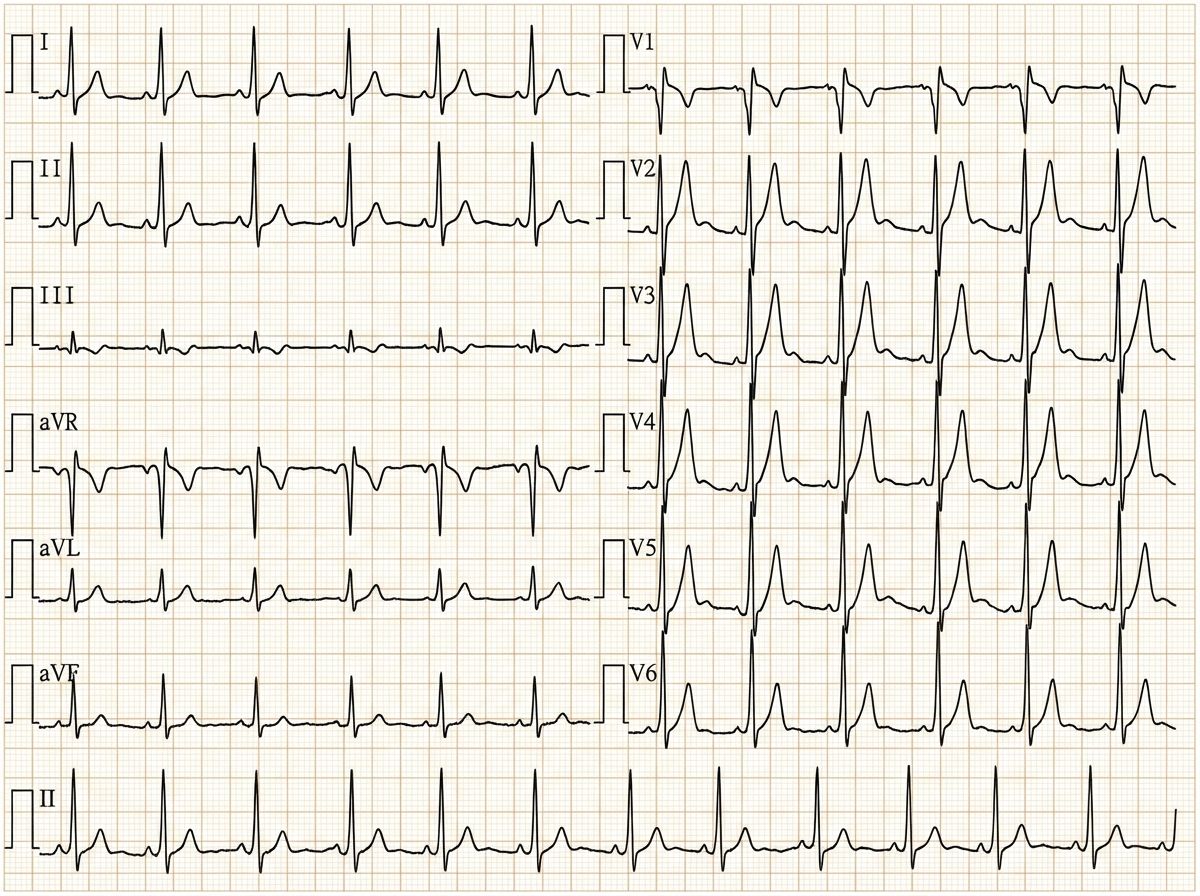
A 29-year-old woman with Wolff-Parkinson-White syndrome presents to her cardiologist’s office for a follow-up visit. She collapsed at her job and made a trip to the emergency department 1 week ago. At that time, she received a diagnosis of atrial fibrillation with rapid ventricular response and hemodynamic instability. While in the emergency department, she underwent direct-current cardioversion to return her heart to sinus rhythm. Her current medications include procainamide. At the cardiologist’s office, her heart rate is 61/min, respiratory rate is 16/min, the temperature is 36.5°C (97.7°F), and blood pressure is 118/60 mm Hg. Her cardiac examination reveals a regular rhythm and a I/VI systolic ejection murmur best heard at the right upper sternal border. An ECG obtained in the clinic is shown. Which of the following is the most appropriate treatment to prevent further episodes of tachyarrhythmia?
A 51-year-old woman with a history of paroxysmal atrial fibrillation comes to the physician for a follow-up visit. She feels well and wants to discuss pausing her only current medication, flecainide. Her pulse is 75/min and regular, blood pressure is 125/75 mm Hg. Physical examination shows no abnormalities. An ECG shows a PR interval of 180 ms, QRS time of 120 ms, and corrected QT interval of 440 ms. Which of the following ECG changes is most likely to be seen on cardiac stress testing in this patient?
A researcher is studying how electrical activity propagates across the heart. In order to do this, he decides to measure the rate at which an action potential moves within various groups of cardiac muscle tissue. In particular, he isolates fibers from areas of the heart with the following characteristics: A) Dysfunction leads to fixed PR intervals prior to a dropped beat B) Dysfunction leads to increasing PR intervals prior to a dropped beat C) Dysfunction leads to tachycardia with a dramatically widened QRS complex D) Dysfunction leads to tachycardia with a sawtooth pattern on electrocardiogram Which of the following is the proper order of these tissues from fastest action potential propagation to slowest action potential propagation.
A cardiologist is studying how a new virus that infects the heart affects the electrical conduction system of the cardiac myocytes. He decides to obtain electrocardiograms on patients with this disease in order to see how the wave patterns and durations change over time. While studying these records, he asks a medical student who is working with him to interpret the traces. Specifically, he asks her to identify the part that represents initial ventricular depolarization. Which of the following characteristics is most consistent with this feature of the electrocardiogram?
A 50-year-old man with a history of atrial fibrillation presents to his cardiologist’s office for a follow-up visit. He recently started treatment with an anti-arrhythmic drug to prevent future recurrences and reports that he has been feeling well and has no complaints. The physical examination shows that the arrhythmia appears to have resolved; however, there is now mild bradycardia. In addition, the electrocardiogram recording shows a slight prolongation of the PR and QT intervals. Which of the following drugs was most likely used to treat this patient?
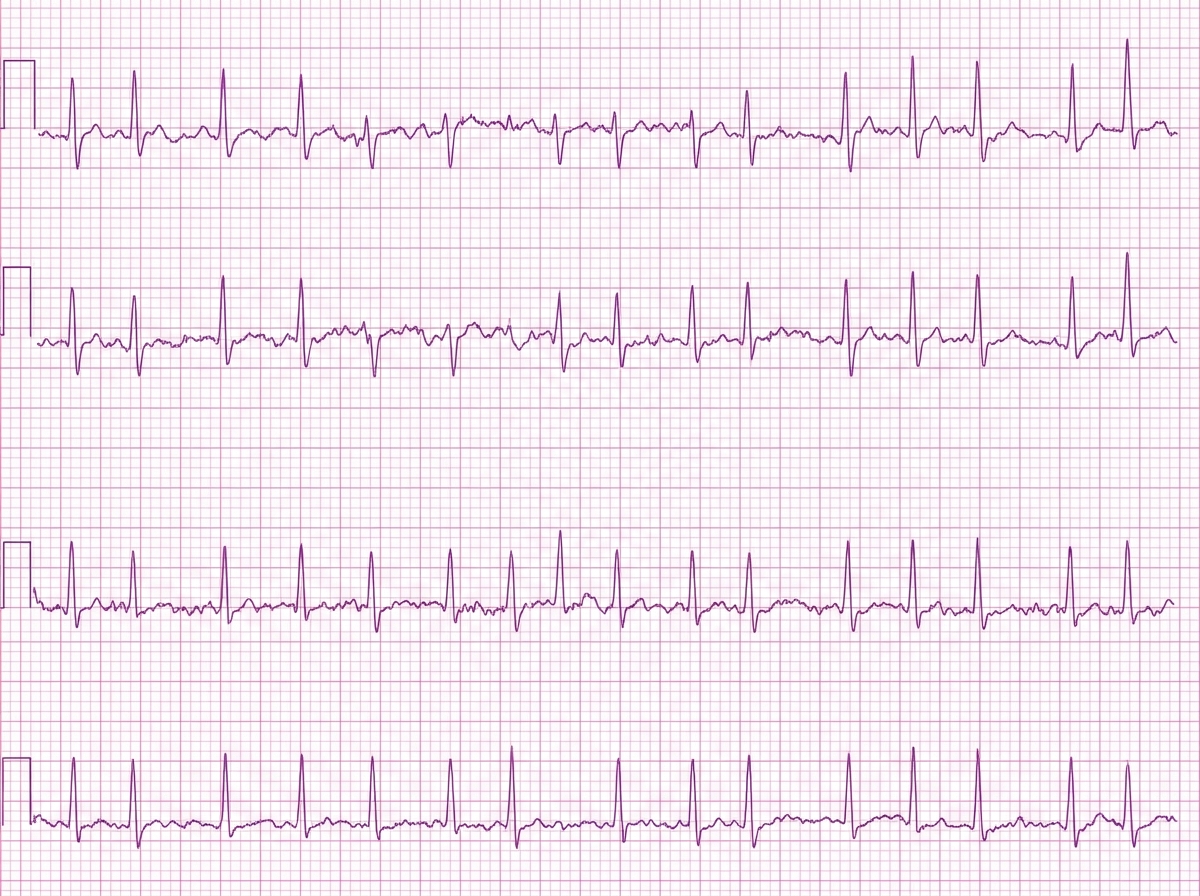
A 42-year-old woman comes to the physician because of a 5-day history of intermittent palpitations. She has no history of syncope or chest pain. She had similar symptoms 1 year ago and following workup has been treated with daily flecainide since then. She drinks one to two glasses of wine on the weekends. She does not smoke. Her pulse is 71/min and her blood pressure is 134/72 mm Hg. A complete blood count shows no abnormalities. Serum creatinine, electrolytes, and TSH are within normal limits. An ECG is shown. Ablation near which of the following sites would be most appropriate for long-term management of this patient's condition?
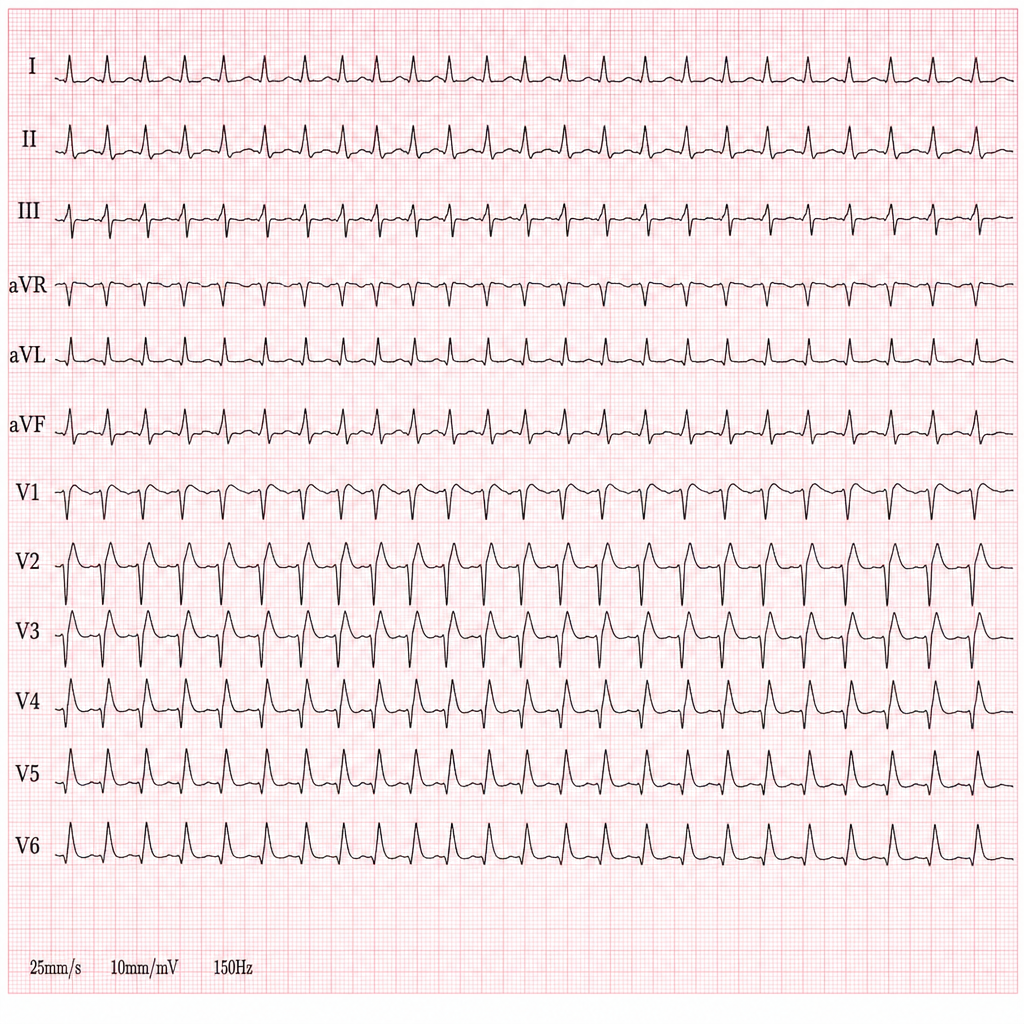
A 44-year-old woman presents with palpitations and lightheadedness. She says that symptoms onset 3 days ago and have not improved. She denies any similar episodes in this past. Her blood pressure is 140/90 mm Hg, heart rate is 150/min, respiratory rate is 16/min, and temperature is 36.6℃ (97.9℉). An ECG is performed and the results are shown in the picture. For cardioversion, it is decided to use an antiarrhythmic agent which has a use-dependent effect. Which of the following medications was most probably used?
A 40-year-old woman comes to the physician for a 6-month history of recurrent episodes of chest pain, racing pulse, dizziness, and difficulty breathing. The episodes last up to several minutes. She also reports urinary urgency and two episodes of loss of consciousness followed by spontaneous recovery. There is no personal or family history of serious illness. She does not smoke or drink alcohol. Vitals signs are within normal limits. Cardiopulmonary examination shows no abnormalities. Holter monitoring is performed. ECG recordings during episodes of tachycardia show a QRS duration of 100 ms, regular RR-interval, and absent P waves. Which of the following is the most likely underlying cause of this patient's condition?
The rapid response team is called for a 74-year-old woman on an inpatient surgical floor for supraventricular tachycardia. The patient had surgery earlier in the day for operative management of a femur fracture. The patient has a history of hypertension, atherosclerosis, type 2 diabetes, and uterine cancer status post total abdominal hysterectomy 20 years prior. With carotid massage, valsalva maneuvers, and metoprolol, the patient breaks out of her supraventricular tachycardia. Thirty minutes later, the nurse notices a decline in the patient’s status. On exam, the patient has a temperature of 98.4°F (36.9°C), blood pressure of 102/74 mmHg, pulse of 86/min, and respirations are 14/min. The patient is now dysarthric with noticeable right upper extremity weakness of 2/5 in elbow flexion and extension. All other extremities demonstrate normal strength and sensation. Which of the following most likely contributed to this decline?
A 58-year-old man is diagnosed with right lower lobe pneumonia and has been admitted to a tertiary care hospital. His laboratory investigations suggest that he acquired an infection from the hospital where he underwent an elective abdominal surgery 3 weeks ago. His past medical records reveal a history of deep vein thrombosis and pulmonary embolism one year prior. After a steady clinical improvement over 5 days of inpatient treatment, he develops a cough, breathlessness, and hemoptysis on the 6th day. His temperature is 38.6°C (101.5°F), the pulse is 112/min, the blood pressure is 130/84 mm Hg, and the respiratory rate is 28/min. A general examination shows the presence of edema over the right leg and tenderness over the right calf region. Auscultation of the chest reveals localized crackles over the left mammary region and right infrascapular region. However, his heart sounds are normal, except for the presence of tachycardia, and there are no murmurs. Which of the following is the investigation of choice as the immediate next step in this patient’s management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app