
Pacemakers and ICDs — MCQs

A 16-year-old male presents to the cardiologist after passing out during a basketball practice. An echocardiogram confirmed the diagnosis of hypertrophic cardiomyopathy. The cardiologist advises that a pacemaker must be implanted to prevent any further complications and states the player cannot play basketball anymore. Unfortunately, the coach objects to sidelining the player since a big game against their rivals is next week. The coach asks if the pacemaker can be implanted after the game, which of the following steps should the physician take?
A 66-year-old female with hypertension and a recent history of acute ST-elevation myocardial infarction (STEMI) 6 days previous, treated with percutaneous transluminal angioplasty (PTA), presents with sudden onset chest pain, shortness of breath, diaphoresis, and syncope. Vitals are temperature 37°C (98.6°F), blood pressure 80/50 mm Hg, pulse 125/min, respirations 12/min, and oxygen saturation 92% on room air. On physical examination, the patient is pale and unresponsive. Cardiac exam reveals tachycardia and a pronounced holosystolic murmur loudest at the apex and radiates to the back. Lungs are clear to auscultation. Chest X-ray shows cardiomegaly with clear lung fields. ECG is significant for ST elevations in the precordial leads (V2-V4) and low-voltage QRS complexes. Emergency transthoracic echocardiography shows a left ventricular wall motion abnormality along with a significant pericardial effusion. The patient is intubated, and aggressive fluid resuscitation is initiated. What is the next best step in management?
A 50-year-old woman presents to the emergency department with mild chest pressure that does not radiate to her left arm or jaw. These episodes have been ongoing several times over the last 24 hours. Her medical history is significant for diabetes mellitus type II and HTN for which she takes metformin and lisinopril. Her physical exam is significant for a middle aged woman appearing as stated age in moderate distress. Her heart and lung sounds are within normal limits. On laboratory examination, her troponin level is elevated, and her heart rate waivers around 47/min. Note this patient’s EKG in the exhibit. Which pacemaker site is likely in use in this patient?
A 67-year-old man presents to the emergency department for squeezing and substernal chest pain. He states that he was at home eating dinner when his symptoms began. The patient has a past medical history of diabetes, hypertension, and dyslipidemia. He is currently taking atorvastatin, lisinopril, insulin, metformin, metoprolol, and aspirin. Six days ago he underwent percutaneous coronary intervention. His temperature is 99.5°F (37.5°C), blood pressure is 197/118 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam reveals an uncomfortable elderly man who is sweating. An ECG is ordered. Which of the following is the best next step in management for this patient?
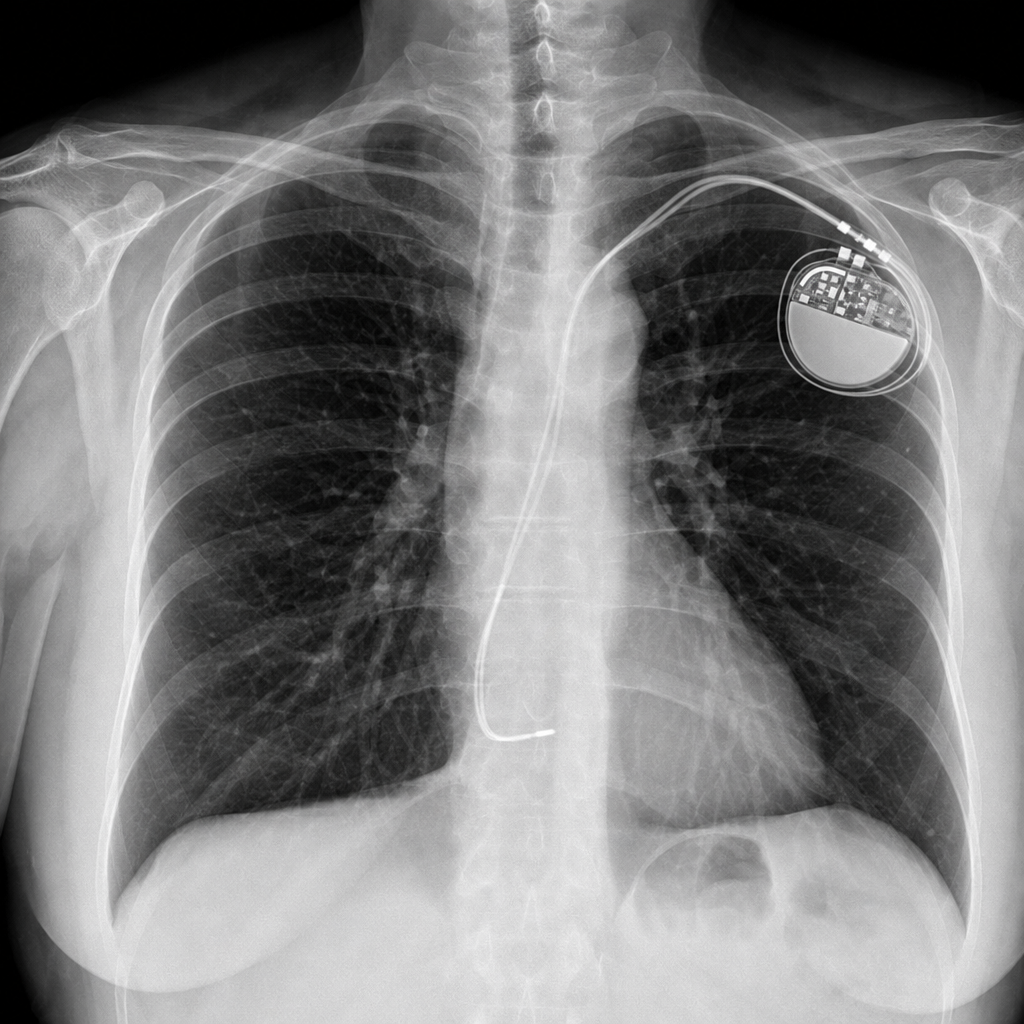
A 67-year-old woman comes to the emergency department because of a 4-month history of fatigue, shortness of breath with exertion, and dizziness. She has a history of atrial fibrillation and had a single-chamber pacemaker placed five years ago after an episode of syncope. Her pulse is 66/min and blood pressure is 98/66 mm Hg. An x-ray of the chest is shown. The x-ray confirms termination of the pacemaker lead in which of the following structures?
A 65-year-old woman is transferred to the intensive care unit after she underwent coronary stenting for a posterior-inferior STEMI. She is known to have allergies to amiodarone and captopril. A few hours after the transfer, she suddenly loses consciousness. The monitor shows ventricular fibrillation. CPR is initiated. After 3 consecutive shocks with a defibrillator, the monitor shows ventricular fibrillation. Which of the following medications should be administered next?
A 71-year-old woman with a past medical history of type 2 diabetes, hypercholesterolemia, and hypertension was admitted to the hospital 8 hours ago with substernal chest pain for management of acute non-ST-elevated myocardial infarction (NSTEMI). The ECG findings noted by ST-depressions and T-wave inversions on anterolateral leads, which is also accompanied by elevated cardiac enzymes. Upon diagnosis, management with inhaled oxygen therapy, beta-blockers and aspirin, and low-molecular-weight heparin therapy were initiated, and she was placed on bed rest with continuous electrocardiographic monitoring. Since admission, she required 2 doses of sublingual nitroglycerin for recurrent angina, and the repeat troponin levels continued to rise. Given her risk factors, plans were made for early coronary angiography. The telemetry nurse calls the on-call physician because of her concern with the patient's mild confusion and increasing need for supplemental oxygen. At bedside evaluation, The vital signs include: heart rate 122/min, blood pressure 89/40 mm Hg, and the pulse oximetry is 91% on 6L of oxygen by nasal cannula. The telemetry and a repeat ECG show sinus tachycardia. She is breathing rapidly, appears confused, and complains of shortness of breath. On physical exam, the skin is cool and clammy and appears pale and dull. She has diffuse bilateral pulmonary crackles, and an S3 gallop is noted on chest auscultation with no new murmurs. She has jugular venous distention to the jaw-line, rapid and faint radial pulses, and 1+ dependent edema. She is immediately transferred to the intensive care unit for respiratory support and precautions for airway security. The bedside sonography shows abnormal hypodynamic anterior wall movement and an ejection fraction of 20%, but no evidence of mitral regurgitation or ventricular shunt. The chest X-ray demonstrates cephalization of pulmonary veins and pulmonary edema. What is the most appropriate next step in the stabilization of this patient?
A 23-year-old man comes to the emergency department because of palpitations, dizziness, and substernal chest pain for three hours. The day prior, he was at a friend’s wedding, where he consumed seven glasses of wine. The patient appears diaphoretic. His pulse is 220/min and blood pressure is 120/84 mm Hg. Based on the patient's findings on electrocardiography, the physician diagnoses atrial fibrillation with rapid ventricular response and administers verapamil for rate control. Ten minutes later, the patient is unresponsive and loses consciousness. Despite resuscitative efforts, the patient dies. Histopathologic examination of the heart at autopsy shows an accessory atrioventricular conduction pathway. Electrocardiography prior to the onset of this patient's symptoms would most likely have shown which of the following findings?
A 54-year-old man with alcoholism comes to the emergency department because of vomiting blood for 6 hours. He has had 3–4 episodes in which he has vomited dark red blood during this period. He has had no epigastric pain or tarry stools. On arrival, his temperature is 37.3°C (99.1°F), pulse is 134/min, and blood pressure is 80/50 mm Hg. He is resuscitated with 0.9% saline and undergoes an emergency upper endoscopy, which shows actively bleeding varices. Band ligation of the varices is done and hemostasis is achieved. He is diagnosed with Child class B cirrhosis. He is concerned about the possibility of recurrence of such an episode. He is asked to abstain from alcohol, to which he readily agrees. In addition to non-selective beta-blocker therapy, which of the following is the most appropriate recommendation to prevent future morbidity and mortality from this condition?
A 54-year-old woman comes to the emergency department because of two episodes of bright red blood per rectum within the past day. She has a history of migraine, which is treated prophylactically with verapamil. She appears well and is hemodynamically stable. Cardiac exam reveals a regular heart rate without any murmurs or gallops. Lungs are clear to auscultation. Her abdomen is mildly tender without rebound or guarding. Digital rectal examination shows fresh blood on the glove. Laboratory studies show: Hemoglobin 10.4 g/dL Leukocyte count 5,000/mm3 Platelet count 175,000/mm3 Partial thromboplastin time 35 seconds Serum Na+ 140 mEq/L K+ 3.7 mEq/L Cl- 101 mEq/L HCO3- 25 mEq/L Mg2+ 1.8 mEq/L A routine ECG shows a heart rate of 75/min, a normal axis, PR interval of 280 ms, QRS interval of 80 ms with a QRS complex following each p wave, and no evidence of ischemic changes. Which of the following is the most appropriate next step in management with respect to this patient's cardiovascular workup?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app