
ECG interpretation fundamentals — MCQs

A 21-year-old woman presents with palpitations and anxiety. She had a recent outpatient ECG that was suggestive of supraventricular tachycardia, but her previous physician failed to find any underlying disease. No other significant past medical history. Her vital signs include blood pressure 102/65 mm Hg, pulse 120/min, respiratory rate 17/min, and temperature 36.5℃ (97.7℉). Electrophysiological studies reveal an atrioventricular nodal reentrant tachycardia. The patient refuses an ablation procedure so it is decided to perform synchronized cardioversion with consequent ongoing management with verapamil. Which of the following ECG features should be monitored in this patient during treatment?
A 75-year-old man presents to the emergency department after an episode of syncope while walking outside with his wife. His wife states that he suddenly appeared pale and collapsed to the ground. She says he remained unconscious for 1 minute. He says he noticed a fluttering in his chest and excessive sweating before the episode. He has type 2 diabetes mellitus, essential hypertension, and chronic stable angina. He has not started any new medications in the past few months. Vital signs reveal: temperature 37.0°C (98.6°F), blood pressure 135/72 mm Hg, and pulse 72/min. Physical examination is unremarkable. ECG shows an old bifascicular block. Echocardiogram and 24-hour Holter monitoring are normal. Which of the following is the best next step in the evaluation of this patient's condition?
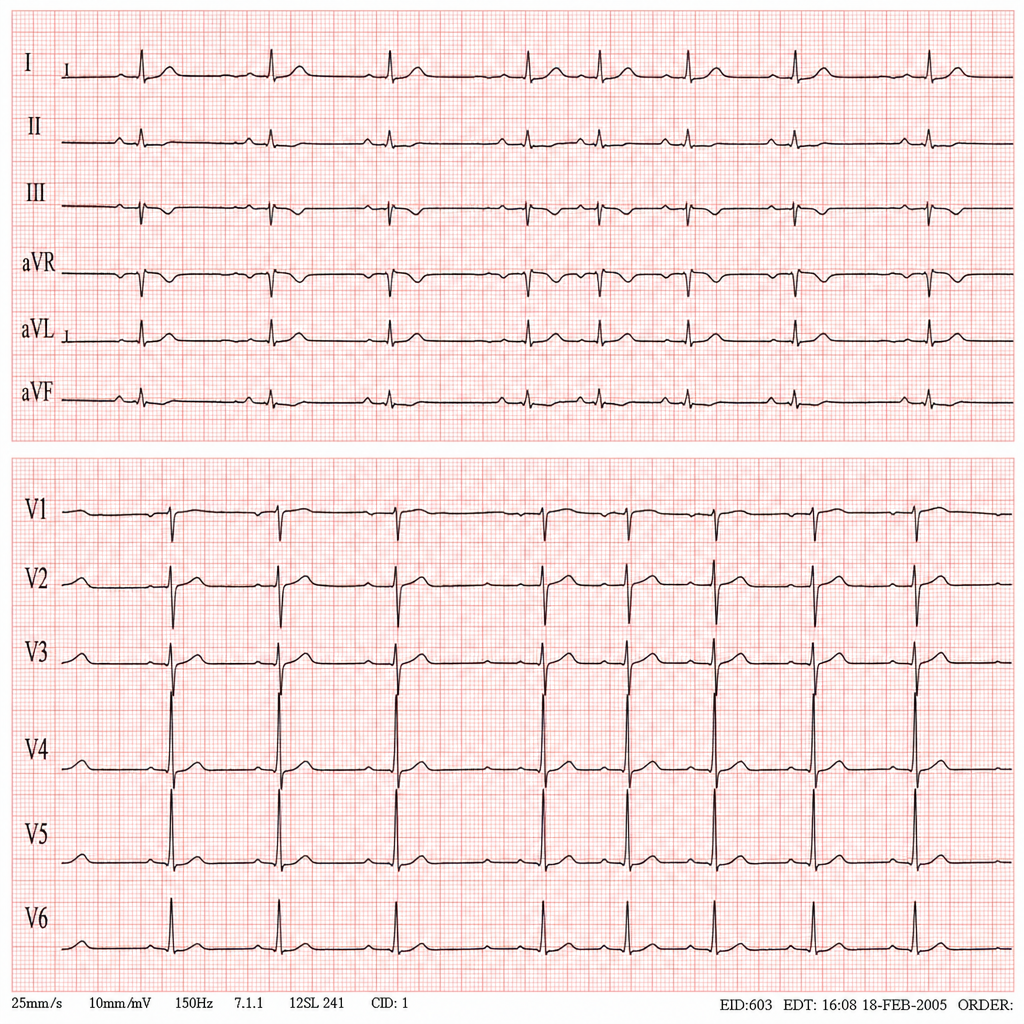
A 45-year-old man comes to the physician for a routine health maintenance examination. He feels well. He underwent appendectomy at the age of 25 years. He has a history of hypercholesterolemia that is well controlled with atorvastatin. He is an avid marathon runner and runs 8 miles per day four times a week. His father died of myocardial infarction at the age of 42 years. The patient does not smoke or drink alcohol. His vital signs are within normal limits. Cardiopulmonary examination shows no abnormalities. His abdomen is soft and nontender with a surgical scar in the right lower quadrant. Laboratory studies are within normal limits. An ECG is shown. Which of the following is the most likely diagnosis?
A 71-year-old man is brought to the emergency department by his wife because of increasing confusion, weakness, and vomiting for 1 day. He has had 5 episodes of vomiting and blurry vision; he told his wife that "everything appears in different colors." He has been unable to recall his wife's name or their address. His wife reports that his drug regimen was adjusted because of worsening tibial edema 1 week ago. He has congestive heart failure, atrial fibrillation, hypothyroidism, and osteoarthritis. Current medications include rivaroxaban, metoprolol, digoxin, levothyroxine, spironolactone, and furosemide. His temperature is 36.7°C (98°F), pulse is 56/min, and blood pressure is 98/68 mm Hg. He is confused and oriented only to person. Neurologic examination shows no focal findings. The abdomen is soft, and there is tenderness to palpation of both lower quadrants without guarding or rebound. There is 1+ pitting edema of both ankles. This patient is most likely to have which of the following ECG findings?
A 72-year-old man comes to the physician because of a 2-month history of intermittent retrosternal chest pain and tightness on exertion. He has type 2 diabetes mellitus, osteoarthritis of the right hip, and hypertension. Current medications include insulin, ibuprofen, enalapril, and hydrochlorothiazide. Vital signs are within normal limits. His troponin level is within the reference range. An ECG at rest shows a right bundle branch block and infrequent premature ventricular contractions. The patient's symptoms are reproduced during adenosine stress testing. Repeat ECG during stress testing shows new ST depression of > 1 mm in leads V2, V3, and V4. Which of the following is the most important underlying mechanism of this patient's ECG changes?
A 41-year-old woman presents to the emergency room with chest pain. She has had progressive substernal chest pain accompanied by weakness and mild shortness of breath for the past 2 hours. Her past medical history is notable for poorly controlled systemic lupus erythematosus (SLE), Sjogren syndrome, and interstitial lung disease. She was hospitalized last year with pericarditis presumed to be from SLE. Her temperature is 98.6°F (37°C), blood pressure is 106/56 mmHg, pulse is 132/min, and respirations are 26/min. On exam, the skin overlying the internal jugular vein fills at 9 cm above the sternal angle and distant heart sounds are appreciated. There is no friction rub. She is given 1000cc of intravenous fluids with no appreciable change in her blood pressure. An electrocardiogram in this patient would most likely reveal which of the following findings?
A 23-year-old man comes to the emergency department because of palpitations, dizziness, and substernal chest pain for three hours. The day prior, he was at a friend’s wedding, where he consumed seven glasses of wine. The patient appears diaphoretic. His pulse is 220/min and blood pressure is 120/84 mm Hg. Based on the patient's findings on electrocardiography, the physician diagnoses atrial fibrillation with rapid ventricular response and administers verapamil for rate control. Ten minutes later, the patient is unresponsive and loses consciousness. Despite resuscitative efforts, the patient dies. Histopathologic examination of the heart at autopsy shows an accessory atrioventricular conduction pathway. Electrocardiography prior to the onset of this patient's symptoms would most likely have shown which of the following findings?
Two days after undergoing an uncomplicated total thyroidectomy, a 63-year-old woman has acute, progressive chest pain. The pain is sharp and burning. She feels nauseated and short of breath. The patient has a history of hypertension, type 1 diabetes mellitus, medullary thyroid cancer, multiple endocrine neoplasia type 2A, anxiety, coronary artery disease, and gastroesophageal reflux disease. She smoked half a pack of cigarettes daily for 24 years but quit 18 years ago. Current medications include lisinopril, insulin glargine, insulin aspart, sertraline, aspirin, ranitidine, and levothyroxine. She appears anxious and diaphoretic. Her temperature is 37.4°C (99.3°F), pulse is 64/min, respirations are 17/min, and blood pressure is 148/77 mm Hg. The lungs are clear to auscultation. Examination shows a 3-cm linear incision over the anterior neck with 1 mm of surrounding erythema and mild serous discharge. The chest wall and abdomen are nontender. There is 5/5 strength in all extremities and decreased sensation to soft touch on the feet bilaterally. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?
A 30-year-old man is brought into the emergency room for complaints of acute onset chest pain and shortness of breath. He has a history of mental retardation and lives at home with his adoptive parents. His parents inform you that he has not seen a doctor since he was adopted as child and that he currently takes no medications. The patient's temperature is 99.1°F (37.3°C), pulse is 108/min, blood pressure is 125/70 mmHg, respirations are 25/min, and oxygen saturation is 92% on 2L nasal cannula. Physical exam is notable for a tall, thin individual with high-arched feet and mild pectus excavatum. There is mild asymmetry in the lower extremities with discomfort to dorsiflexion of the larger leg. Lung auscultation reveals no abnormalities. What is the most appropriate next step in management?
A 40-year-old woman comes to the physician for a 6-month history of recurrent episodes of chest pain, racing pulse, dizziness, and difficulty breathing. The episodes last up to several minutes. She also reports urinary urgency and two episodes of loss of consciousness followed by spontaneous recovery. There is no personal or family history of serious illness. She does not smoke or drink alcohol. Vitals signs are within normal limits. Cardiopulmonary examination shows no abnormalities. Holter monitoring is performed. ECG recordings during episodes of tachycardia show a QRS duration of 100 ms, regular RR-interval, and absent P waves. Which of the following is the most likely underlying cause of this patient's condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app