
Catheter ablation procedures — MCQs

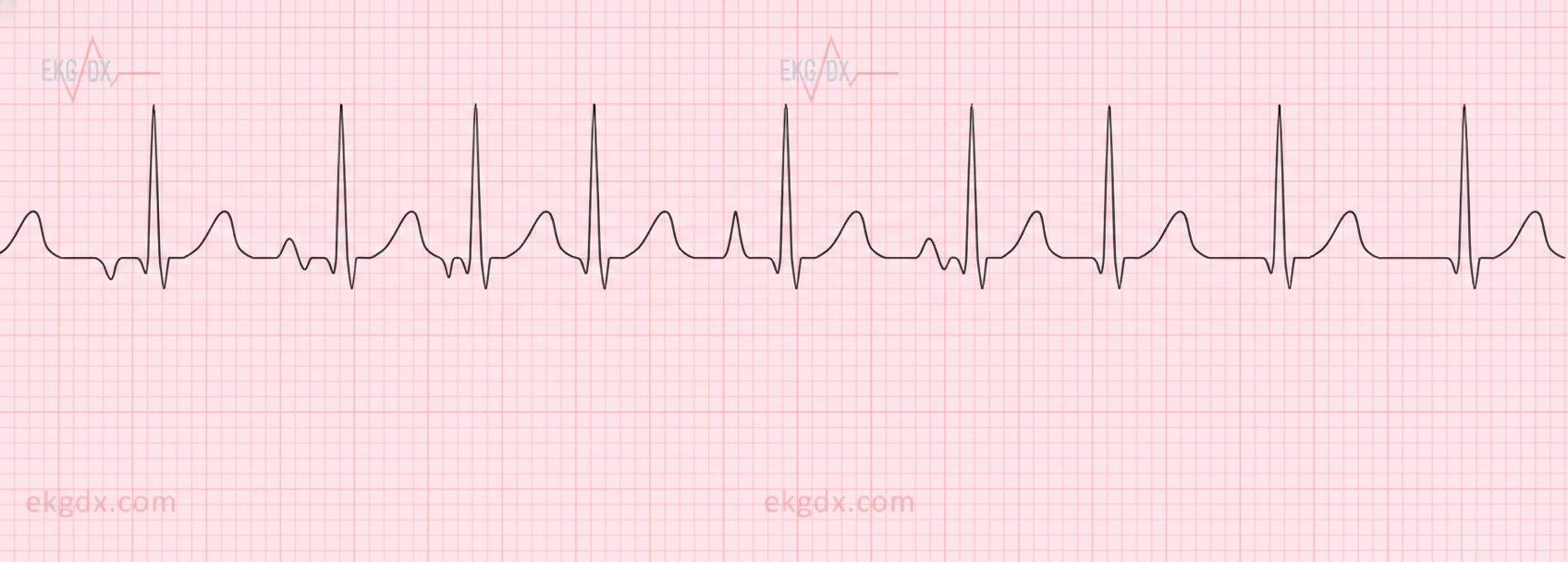
A 44-year-old man comes to the emergency department because of persistent palpitations for the past 2 hours. The day before, he was at a wedding, where he drank several glasses of wine and 9–10 vodka cocktails. He has never had similar symptoms before. He is a manager at a software company and has recently had a lot of work-related stress. He is otherwise healthy and takes no medications. His temperature is 36.5°C (97.7°F), pulse is 90/min and irregularly irregular, respirations are 13/min, and his blood pressure is 128/60 mm Hg. Physical examination shows no other abnormalities. An ECG is performed; no P-waves can be identified. Echocardiography shows no valvular abnormalities and normal ventricular function. One hour later, a repeat ECG shows normal P waves followed by narrow QRS complexes. He is still experiencing occasional palpitations. Which of the following is the most appropriate next step in management?
A 21-year-old woman presents with palpitations and anxiety. She had a recent outpatient ECG that was suggestive of supraventricular tachycardia, but her previous physician failed to find any underlying disease. No other significant past medical history. Her vital signs include blood pressure 102/65 mm Hg, pulse 120/min, respiratory rate 17/min, and temperature 36.5℃ (97.7℉). Electrophysiological studies reveal an atrioventricular nodal reentrant tachycardia. The patient refuses an ablation procedure so it is decided to perform synchronized cardioversion with consequent ongoing management with verapamil. Which of the following ECG features should be monitored in this patient during treatment?
A 16-year-old male presents to the cardiologist after passing out during a basketball practice. An echocardiogram confirmed the diagnosis of hypertrophic cardiomyopathy. The cardiologist advises that a pacemaker must be implanted to prevent any further complications and states the player cannot play basketball anymore. Unfortunately, the coach objects to sidelining the player since a big game against their rivals is next week. The coach asks if the pacemaker can be implanted after the game, which of the following steps should the physician take?
A 64-year-old male presents to the emergency room complaining of chest pain. He reports a pressure-like sensation over his sternum that radiates into his jaw. The pain came on suddenly 2 hours ago and has been constant since then. His past medical history is notable for a stable abdominal aortic aneurysm, hypertension, diabetes, and hyperlipidemia. He takes aspirin, enalapril, spironolactone, atorvastatin, canagliflozin, and metformin. His temperature is 99.1°F (37.3°C), blood pressure is 155/85 mmHg, pulse is 115/min, and respirations are 22/min. On exam, he is diaphoretic and in moderate distress. He is admitted for further management and does well after initial stabilization. He is seen two days later by the admitting team. This patient is at increased risk for a complication that is characterized by which of the following?
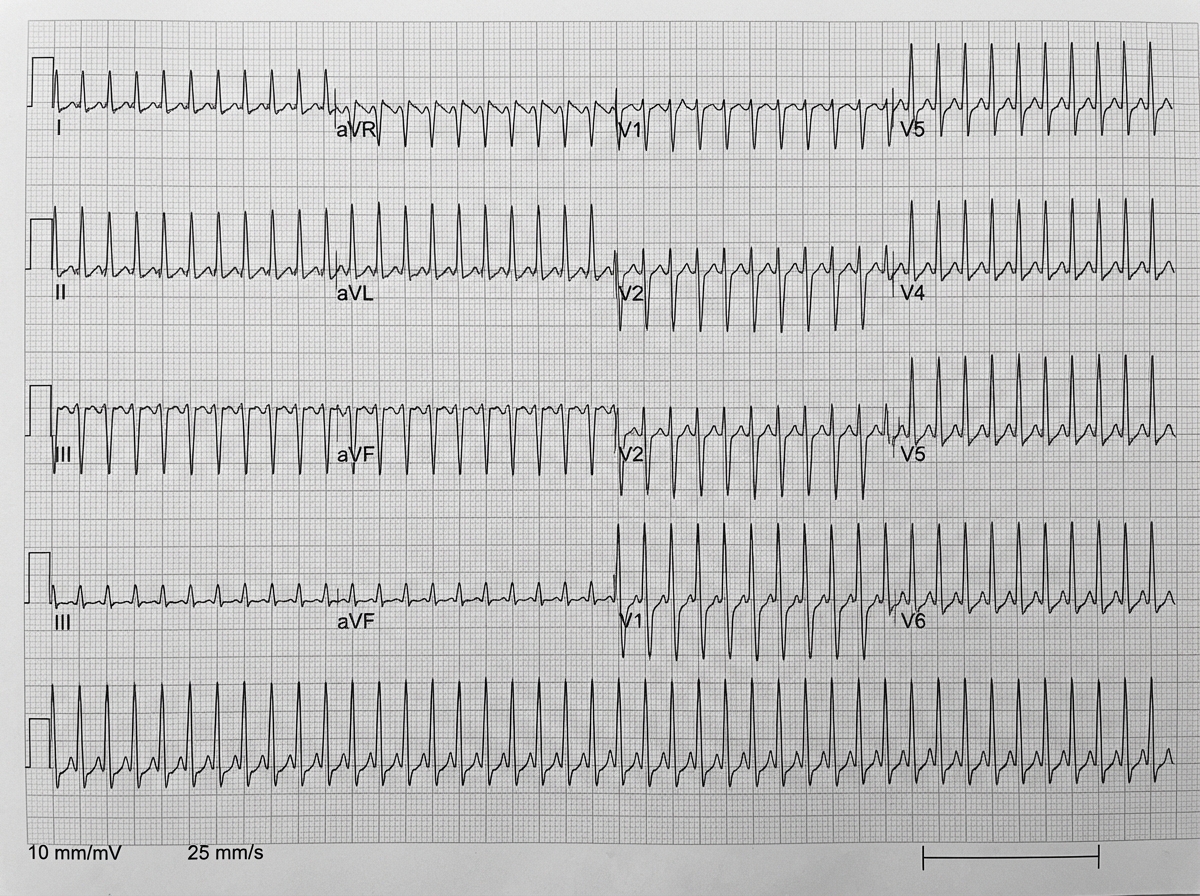
A 62-year-old man with a 5-year history of chronic obstructive pulmonary disease comes to the physician for a follow-up examination. He has had episodic palpitations over the past week. His only medication is a tiotropium-formoterol inhaler. His pulse is 140/min and irregular, respirations are 17/min, and blood pressure is 116/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 95%. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. Serum concentrations of electrolytes, thyroid-stimulating hormone, and cardiac troponins are within the reference range. An electrocardiogram is shown. Which of the following is the most appropriate next step in management?
One week after an aortic valve replacement surgery, a 55-year-old man is brought to the emergency room 30 minutes after the onset of severe, sharp chest pain. He appears pale and dyspneic but is alert, oriented, and speaks in full sentences. His temperature is 38°C (100.4°F), pulse is 192/min and thready, respirations are 22/min, and blood pressure is 80/50 mm Hg. Faint rales can be heard in the lower lung fields on both sides on auscultation. There is a midline thoracotomy scar with mild reddening but without warmth or discharge. A portion of an ECG is shown. The pattern remains unchanged after 1 minute. Which of the following is the most appropriate intervention?
A 43-year-old man comes to the physician because of increasing shortness of breath for 1 month. He has been using two pillows at night but frequently wakes up feeling as if he is choking. Five months ago, he underwent surgery for creation of an arteriovenous fistula in his left upper arm. He has hypertension and chronic kidney disease due to reflux nephropathy. He receives hemodialysis three times a week. His current medications are enalapril, vitamin D3, erythropoietin, sevelamer, and atorvastatin. His temperature is 37.1°C (98.8°F), respirations are 22/min, pulse is 103/min and bounding, and blood pressure is 106/58 mm Hg. Examination of the lower extremities shows bilateral pitting pedal edema. There is jugular venous distention. A prominent thrill is heard over the brachiocephalic arteriovenous fistula. There are crackles heard at both lung bases. Cardiac examination shows an S3 gallop. The abdomen is soft and nontender. Which of the following is the most likely cause of this patient's symptoms?
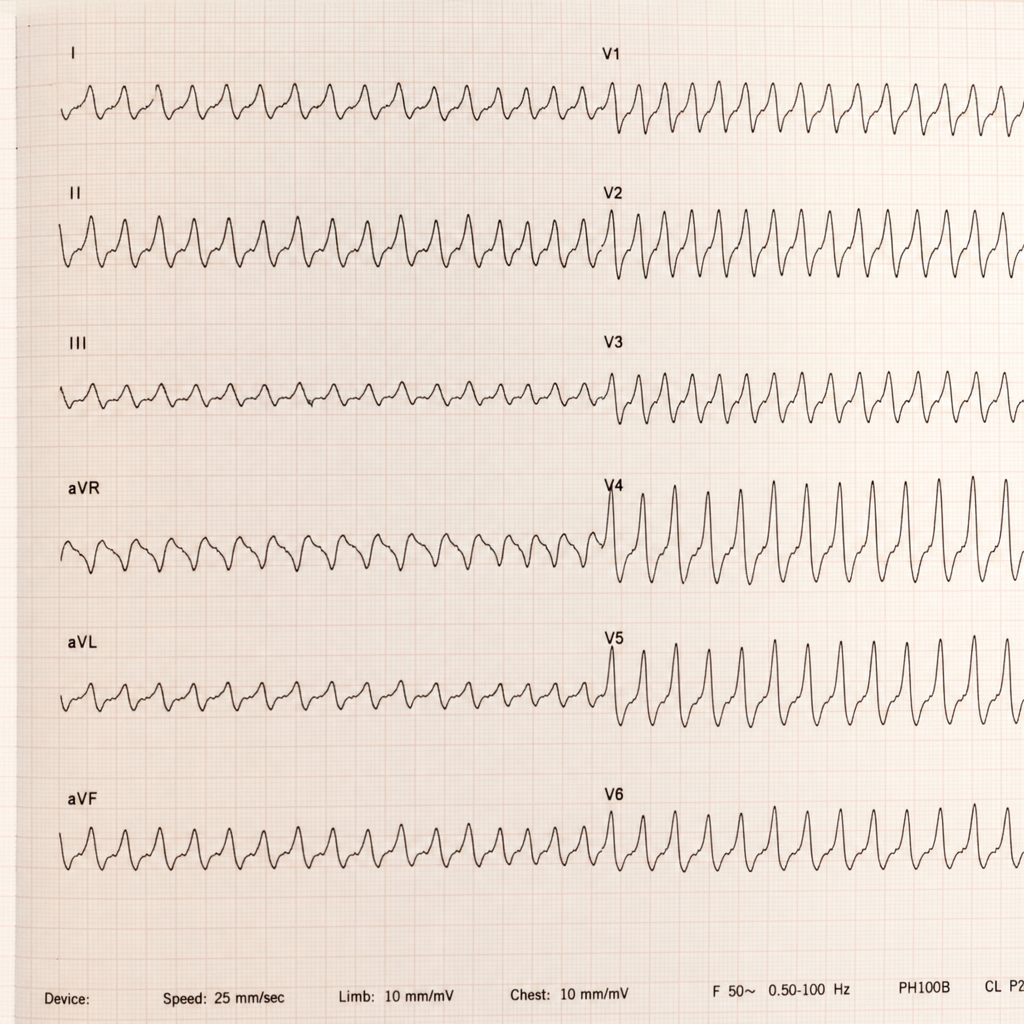
A 26-year-old healthy woman presents with lightheadedness, palpitations, and sweating, which started suddenly after she was frightened by her neighbor’s dog. The patient’s blood pressure is 135/80 mm Hg, the heart rate is 150/min, the respiratory rate is 15/min, and the temperature is 36.6℃ (97.9℉). Her ECG is shown in the exhibit. What is the preferred agent for pharmacologic management of this condition?
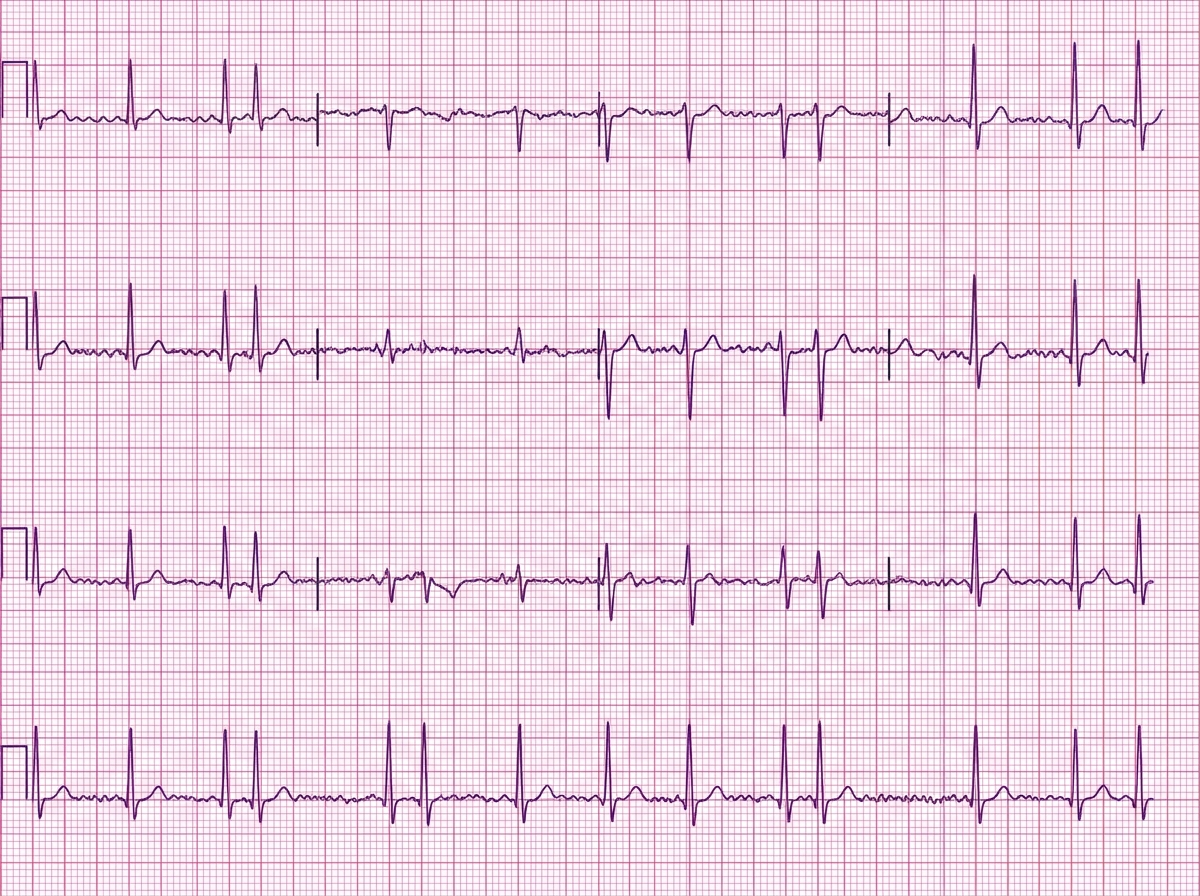
A 77-year-old man presents to the emergency department complaining of feeling like “his heart was racing” for the last 8 days. He denies any chest pain, dizziness, or fainting but complains of fatigue, difficulty breathing with exertion, and swelling of his legs bilaterally for the last 2 weeks. He has had hypertension for the last 25 years. He has a long history of heavy alcohol consumption but denies smoking. His blood pressure is 145/70 mm Hg and the pulse is irregular at the rate of 110/min. On examination of his lower limbs, mild pitting edema is noted of his ankles bilaterally. On cardiac auscultation, heart sounds are irregular. Bibasilar crackles are heard with auscultation of the lungs. An ECG is ordered and the result is shown in the image. Transesophageal echocardiography shows a reduced ejection fraction of 32% and dilatation of all chambers of the heart without any obvious intracardiac thrombus. Which of the following is the optimal therapy for this patient?
A 47-year-old woman comes to the emergency department after coughing up 2 cups of bright red blood. A CT angiogram of the chest shows active extravasation from the right bronchial artery. A coil embolization is planned to stop the bleeding. During this procedure, a catheter is first inserted into the right femoral artery. Which of the following represents the correct subsequent order of the catheter route?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app