
Cardioversion and defibrillation — MCQs

A 55-year-old man presents to his physician with a complaint of recurrent episodes of palpitations over the past 2 weeks. He also mentions that he tends to tire easily. He denies chest pain, breathlessness, dizziness, or syncope, but has a history of ischemic heart disease. He smokes 1 pack of cigarettes every day and drinks alcohol occasionally. The physical examination revealed a temperature of 36.9°C (98.4°F), a pulse of 124/min (irregular), a blood pressure of 142/86 mm Hg, and a respiratory rate of 16/min. Auscultation of his chest is normal with an absence of rales overall lung fields. An ECG was significant for fibrillatory waves and an irregular RR interval. Thus, the physician concludes that the symptoms are due to atrial fibrillation. The patient is prescribed oral diltiazem. Which of the following side effects should the physician warn the patient about?
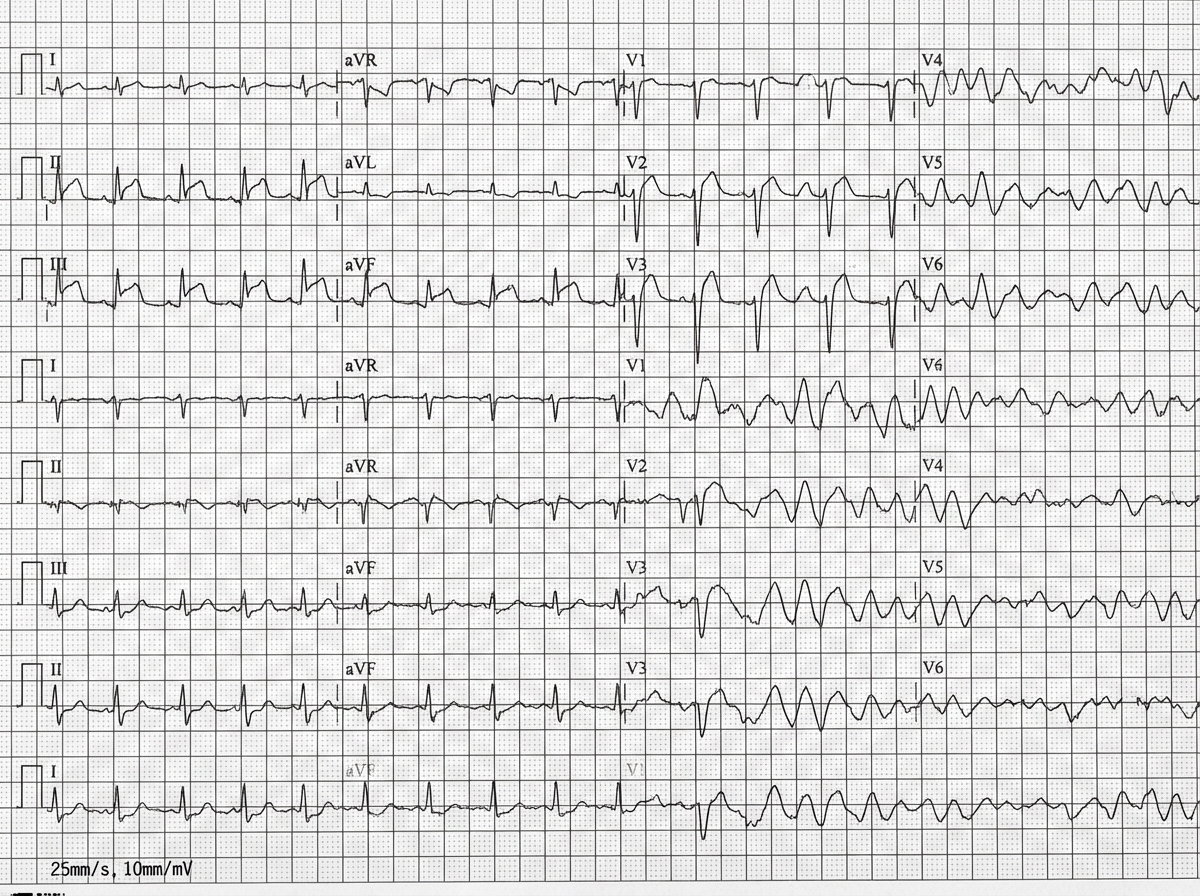
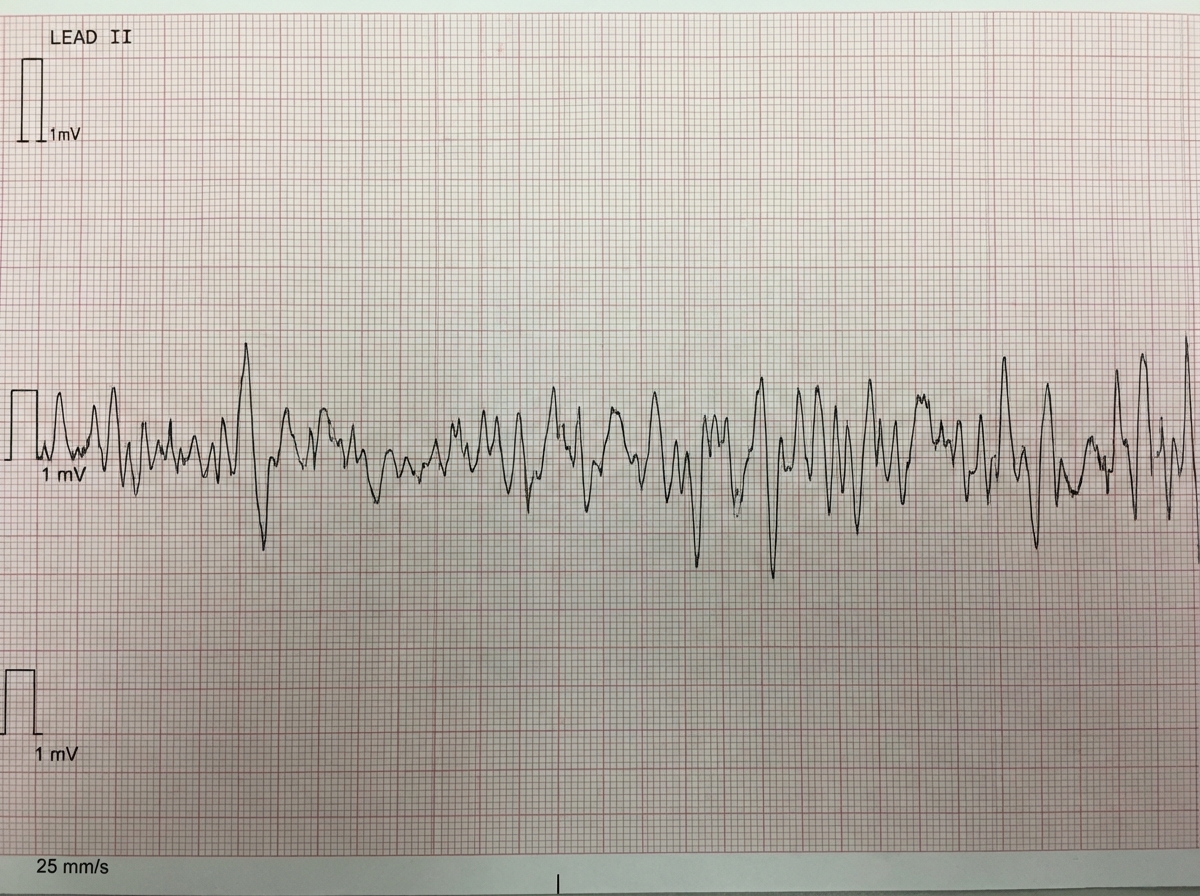
A 42-year-old man is brought to the emergency department 20 minutes after the sudden onset of severe chest pain, diaphoresis, shortness of breath, and palpitations. His symptoms occurred while he was at a party with friends. He has smoked one pack of cigarettes daily for 24 years. He uses cocaine occasionally. The last use was three hours ago. He appears pale. His pulse is 110/min, blood pressure is 178/106 mm Hg, and respirations are 24/min. His pupils are dilated and react sluggishly to light. The lungs are clear to auscultation. An ECG shows tachycardia and ST segment elevation in leads II, III, and aVF. While recording the ECG, the patient loses consciousness. A photo of the ECG at that point is shown. Which of the following is the most appropriate next step in management?
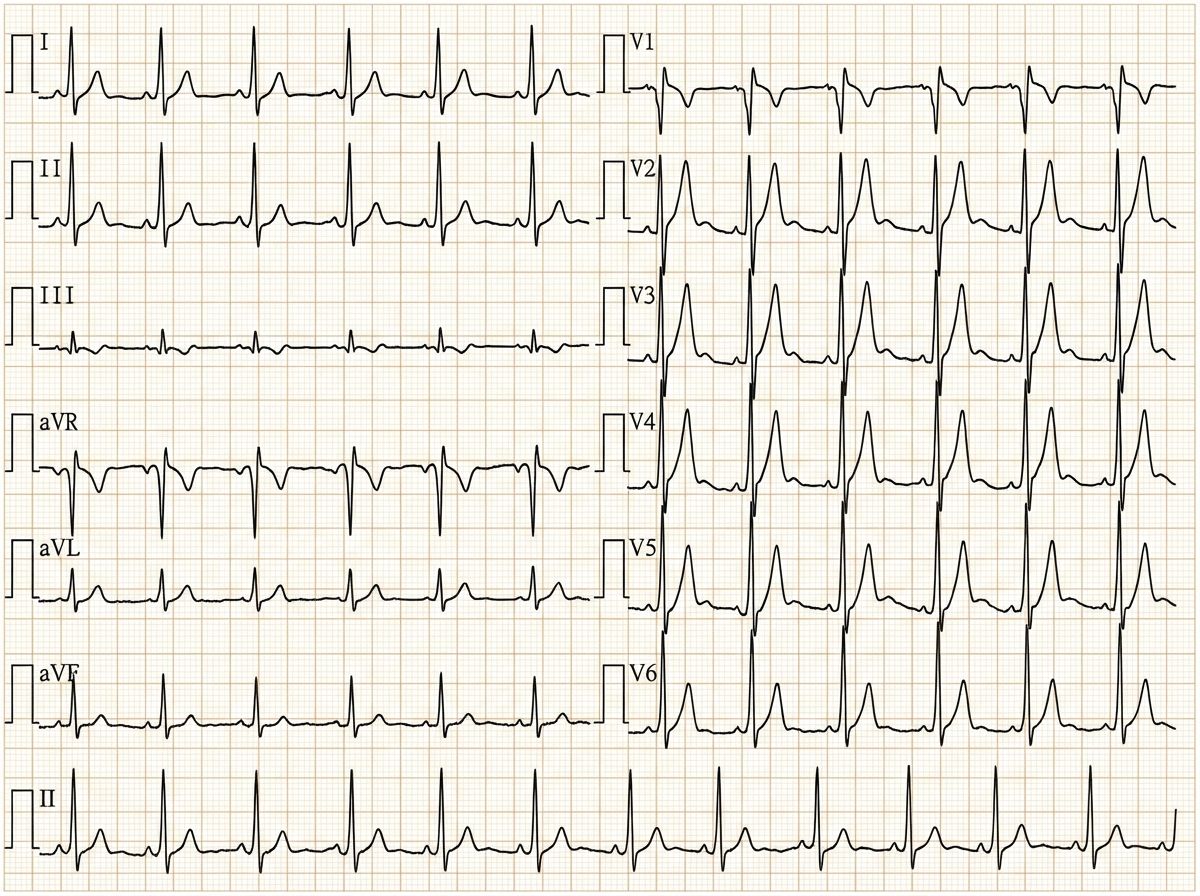
A 29-year-old woman with Wolff-Parkinson-White syndrome presents to her cardiologist’s office for a follow-up visit. She collapsed at her job and made a trip to the emergency department 1 week ago. At that time, she received a diagnosis of atrial fibrillation with rapid ventricular response and hemodynamic instability. While in the emergency department, she underwent direct-current cardioversion to return her heart to sinus rhythm. Her current medications include procainamide. At the cardiologist’s office, her heart rate is 61/min, respiratory rate is 16/min, the temperature is 36.5°C (97.7°F), and blood pressure is 118/60 mm Hg. Her cardiac examination reveals a regular rhythm and a I/VI systolic ejection murmur best heard at the right upper sternal border. An ECG obtained in the clinic is shown. Which of the following is the most appropriate treatment to prevent further episodes of tachyarrhythmia?
A 22-year-old woman presents to the emergency department feeling lightheaded and states that her heart is racing. She does not have a history of any chronic medical conditions. She is a college sophomore and plays club volleyball. Although she feels stressed about her upcoming final exams next week, she limits her caffeine intake to 3 cups of coffee per day to get a good night sleep. She notes that her brother takes medication for some type of heart condition, but she does not know the name of it. Both her parents are alive and well. She denies recent illness, injuries, or use of cigarettes, alcohol, or recreational drugs. The pertinent negatives from the review of systems include an absence of fever, nausea, vomiting, sweating, fatigue, or change in bowel habits. The vital signs include: temperature 36.8°C (98.2°F), heart rate 125/min, respiratory rate 15/min, blood pressure 90/75 mm Hg, and oxygen saturation of 100% on room air. The laboratory results are within normal limits. The ECG is significant for a shortened PR interval and widened QRS. Which of the following medications should the patient avoid in this scenario?
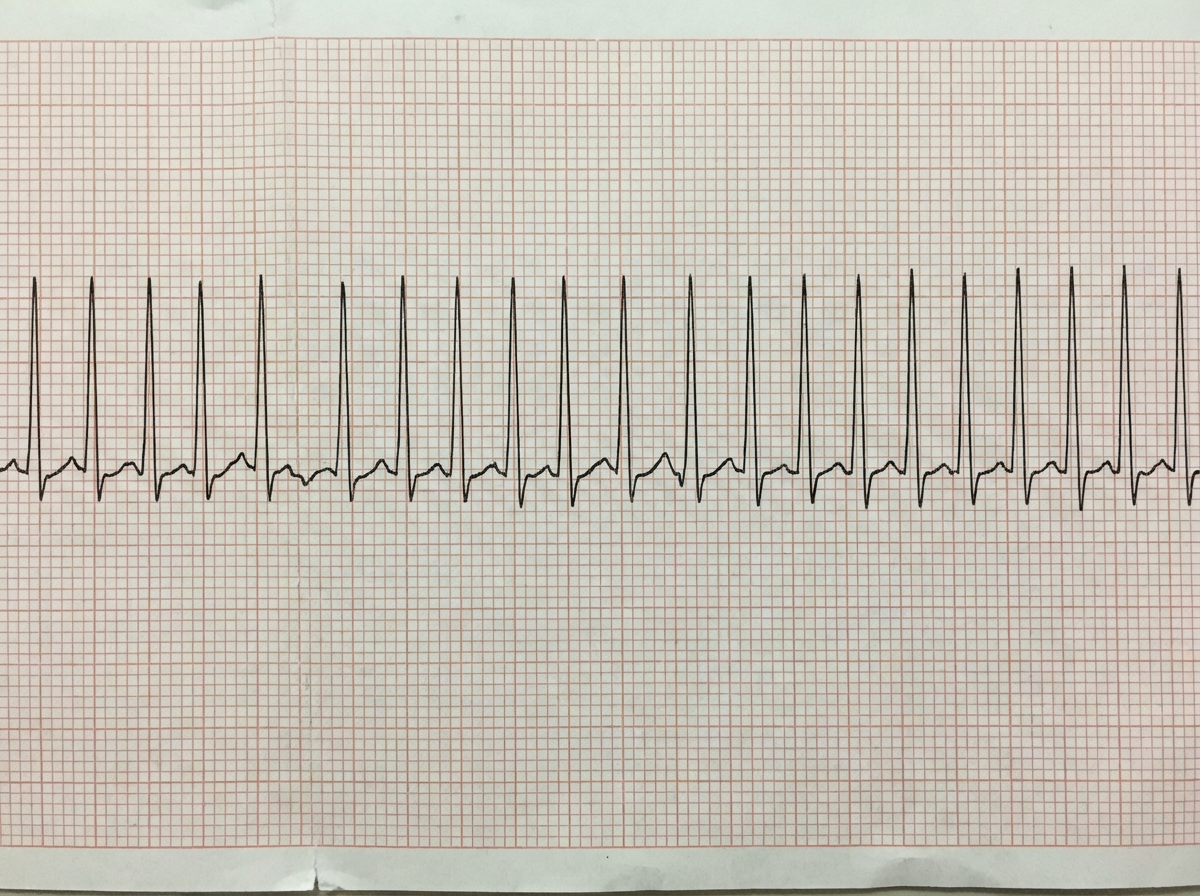
A previously healthy 33-year-old woman comes to the emergency department because she could feel her heart racing intermittently for the last 2 hours. Each episode lasts about 10 minutes. She does not have any chest pain. Her mother died of a heart attack and her father had an angioplasty 3 years ago. She has smoked a half pack of cigarettes daily for 14 years. She drinks one to two beers daily. She appears anxious. Her temperature is 37.6°C (98.1°F), pulse is 160/min, and blood pressure is 104/76 mm Hg. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. An ECG is shown. Which of the following is the most appropriate initial step in management?
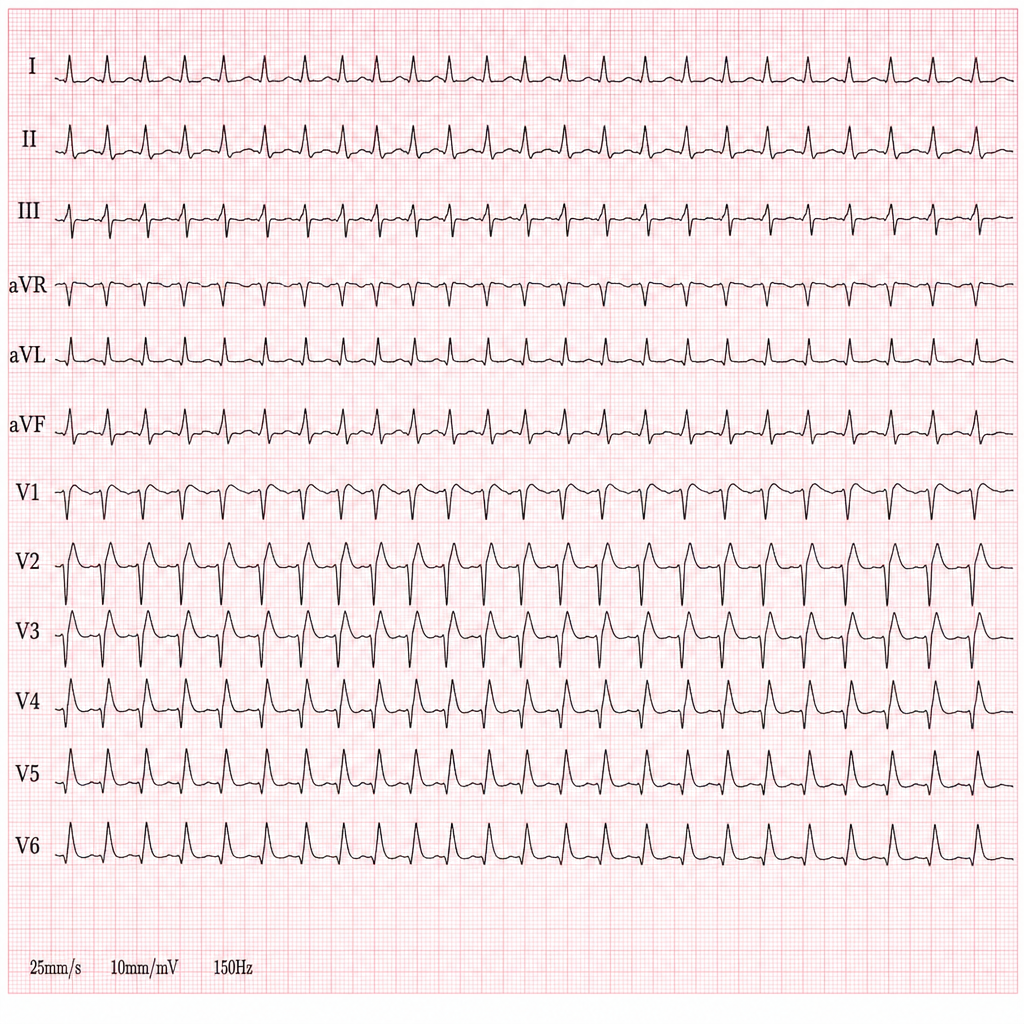
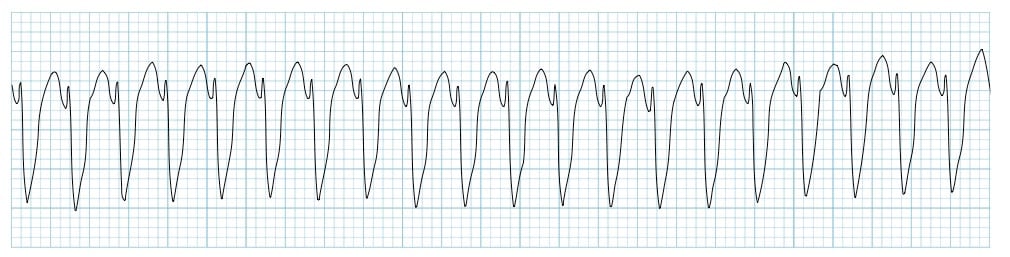
A 44-year-old woman presents with palpitations and lightheadedness. She says that symptoms onset 3 days ago and have not improved. She denies any similar episodes in this past. Her blood pressure is 140/90 mm Hg, heart rate is 150/min, respiratory rate is 16/min, and temperature is 36.6℃ (97.9℉). An ECG is performed and the results are shown in the picture. For cardioversion, it is decided to use an antiarrhythmic agent which has a use-dependent effect. Which of the following medications was most probably used?
Two days after admission for myocardial infarction and subsequent coronary angioplasty, a 65-year-old man becomes distressed and diaphoretic in the cardiac intensive care unit. Suddenly he is no longer responsive. Pulse oximetry does not show a tracing. He has a history of hypertension and depression. Prior to his admission, his medication included ramipril and aripiprazole. Examination shows no carotid pulse. An ECG is shown. After beginning chest compressions, which of the following is the most appropriate step in management of the patient?
One hour after being admitted to the hospital for sharp, acute chest pain and diaphoresis, a 55-year-old woman with type 2 diabetes mellitus loses consciousness in the emergency department. There are no palpable pulses. Chest compressions are started. The patient has a history of breast cancer that was surgically treated 4 years ago. Prior to admission, the patient was on a long bus ride to visit her sister. Her medications include tamoxifen, atorvastatin, metoprolol, metformin, and insulin. Serum troponin levels are elevated. The cardiac rhythm is shown. Which of the following is the most appropriate next step in management?
Two days after coronary artery stent placement for a posterior myocardial infarction, a 70-year-old woman complains of difficulty breathing and retrosternal chest pain. She has a history of atrial fibrillation, for which she takes verapamil. Following stent placement, the patient was started on aspirin and clopidogrel. She appears to be in acute distress and is disoriented. Respirations are 22/min. Pulse oximetry on room air shows an oxygen saturation of 80%. Diffuse crackles are heard on auscultation of the chest. The patient is intubated and mechanical ventilation is started. Shortly afterwards, she becomes unresponsive. Heart sounds are inaudible and her carotid pulses are not palpable. The cardiac monitor shows normal sinus rhythm with T-wave inversion. Which of the following is the most appropriate next step in management?
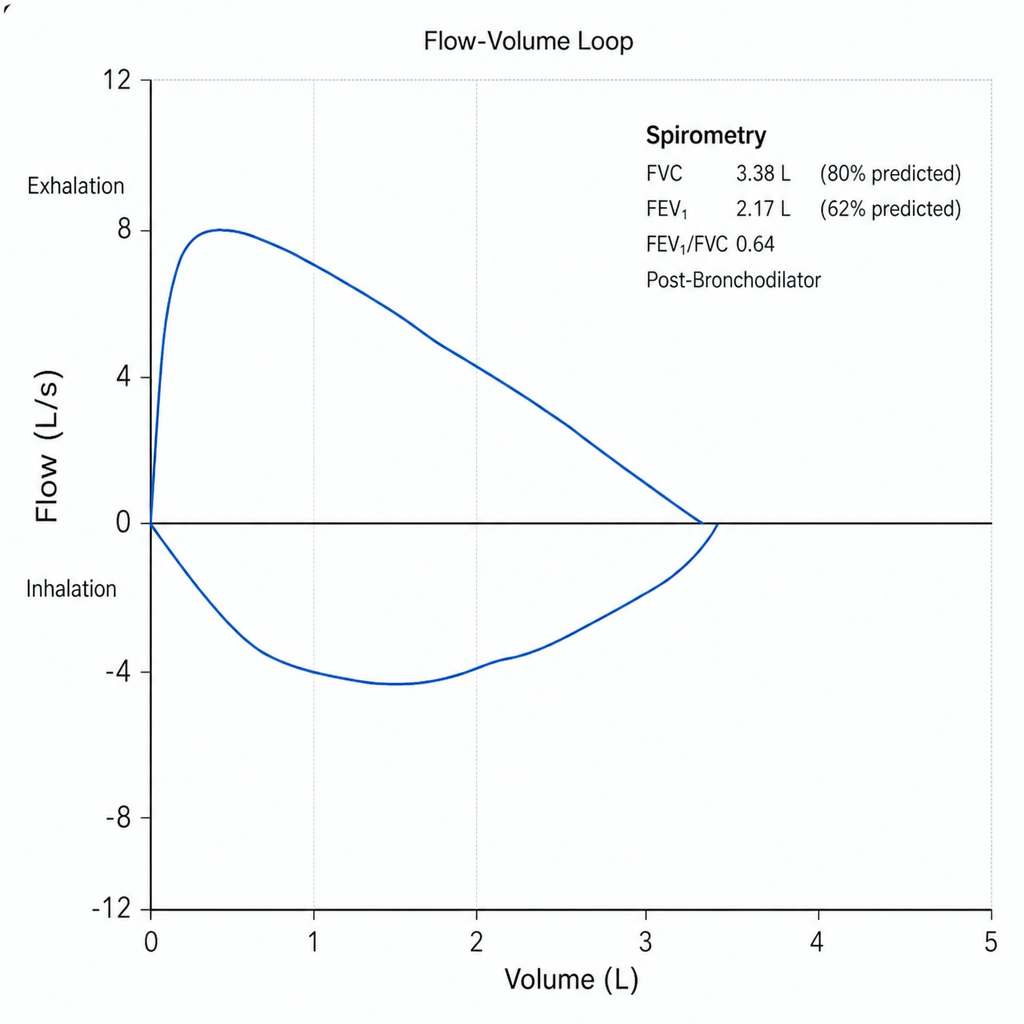
A 58-year-old man with a 40 pack-year smoking history presents with progressive dyspnea over 8 months, a chronic productive cough, and two hospitalizations for respiratory infections in the past year. He uses albuterol as needed with partial relief. Spirometry is performed and the flow-volume loop is shown below. Post-bronchodilator FEV₁/FVC is 0.64 and FEV₁ is 62% of predicted. Which of the following best describes the physiologic pattern and the most appropriate escalation of maintenance therapy?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app