
Atrial fibrillation and flutter — MCQs

A 21-year-old woman presents with palpitations and anxiety. She had a recent outpatient ECG that was suggestive of supraventricular tachycardia, but her previous physician failed to find any underlying disease. No other significant past medical history. Her vital signs include blood pressure 102/65 mm Hg, pulse 120/min, respiratory rate 17/min, and temperature 36.5℃ (97.7℉). Electrophysiological studies reveal an atrioventricular nodal reentrant tachycardia. The patient refuses an ablation procedure so it is decided to perform synchronized cardioversion with consequent ongoing management with verapamil. Which of the following ECG features should be monitored in this patient during treatment?
A 75-year-old man presents to the emergency department after an episode of syncope while walking outside with his wife. His wife states that he suddenly appeared pale and collapsed to the ground. She says he remained unconscious for 1 minute. He says he noticed a fluttering in his chest and excessive sweating before the episode. He has type 2 diabetes mellitus, essential hypertension, and chronic stable angina. He has not started any new medications in the past few months. Vital signs reveal: temperature 37.0°C (98.6°F), blood pressure 135/72 mm Hg, and pulse 72/min. Physical examination is unremarkable. ECG shows an old bifascicular block. Echocardiogram and 24-hour Holter monitoring are normal. Which of the following is the best next step in the evaluation of this patient's condition?
A 26-year-old nursing home staff presents to the emergency room with complaints of palpitations and chest pain for the past 2 days. She was working at the nursing home for the last year but has been trying to get into modeling for the last 6 months and trying hard to lose weight. She is a non-smoker and occasionally drinks alcohol on weekends with friends. On examination, she appears well nourished and is in no distress. The blood pressure is 150/84 mm Hg and the pulse is 118/min. An ECG shows absent P waves. All other physical findings are normal. What is the probable diagnosis?
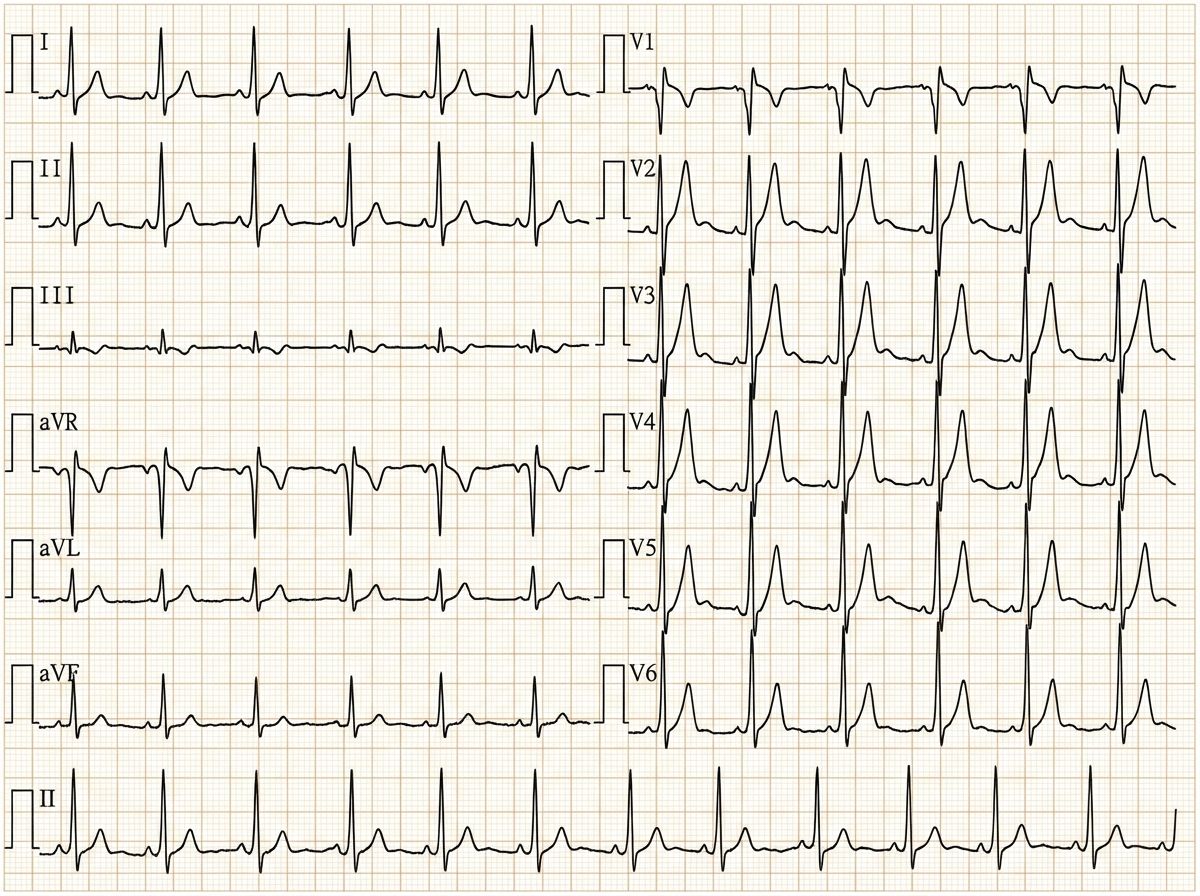
A 29-year-old woman with Wolff-Parkinson-White syndrome presents to her cardiologist’s office for a follow-up visit. She collapsed at her job and made a trip to the emergency department 1 week ago. At that time, she received a diagnosis of atrial fibrillation with rapid ventricular response and hemodynamic instability. While in the emergency department, she underwent direct-current cardioversion to return her heart to sinus rhythm. Her current medications include procainamide. At the cardiologist’s office, her heart rate is 61/min, respiratory rate is 16/min, the temperature is 36.5°C (97.7°F), and blood pressure is 118/60 mm Hg. Her cardiac examination reveals a regular rhythm and a I/VI systolic ejection murmur best heard at the right upper sternal border. An ECG obtained in the clinic is shown. Which of the following is the most appropriate treatment to prevent further episodes of tachyarrhythmia?
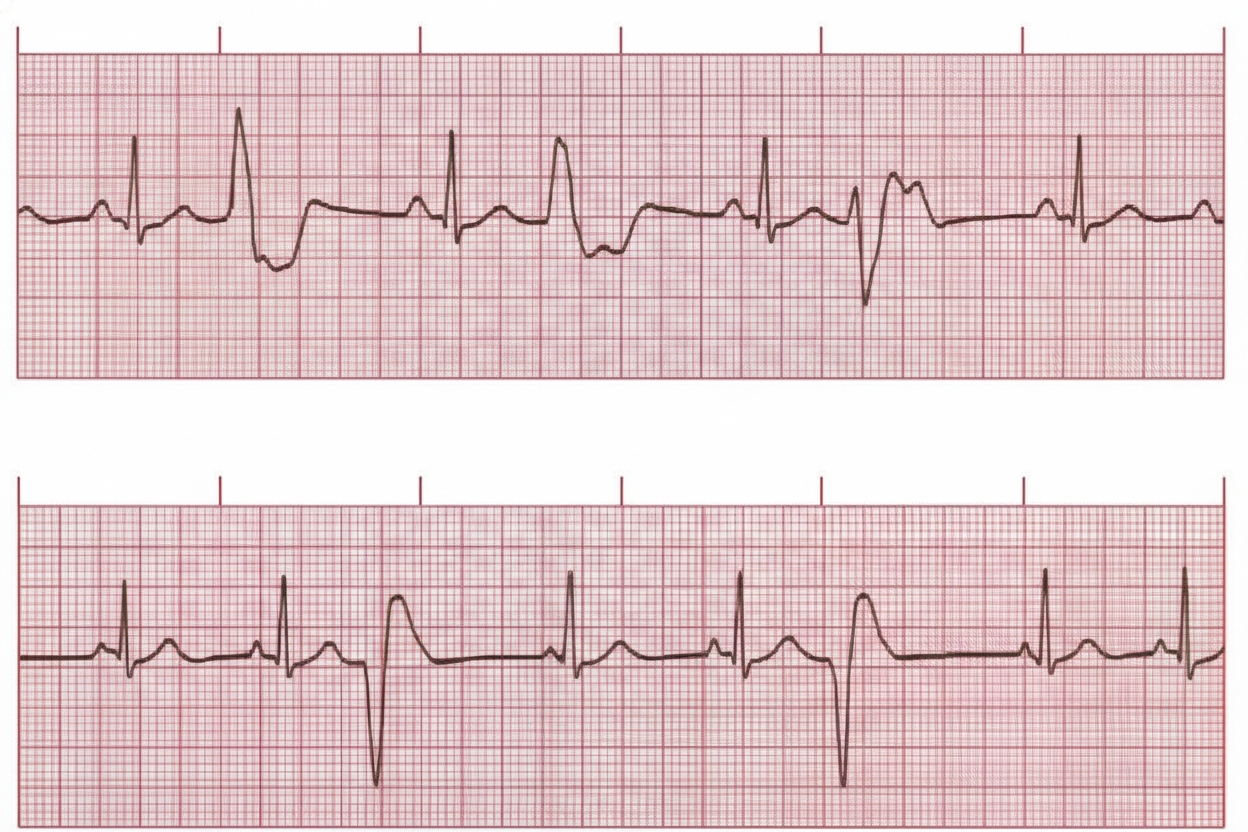
A 24-year-old woman comes to the physician for a routine health maintenance examination. She feels well. On questioning, she has had occasional morning dizziness and palpitations during the past year. She is a graduate student. She does not smoke and drinks 1–2 glasses of wine on the weekends. Her vital signs are within normal limits. Physical examination shows an irregular pulse. On auscultation of the chest, S1 and S2 are normal and there are no murmurs. An ECG is shown. Which of the following is the most appropriate next step in management?
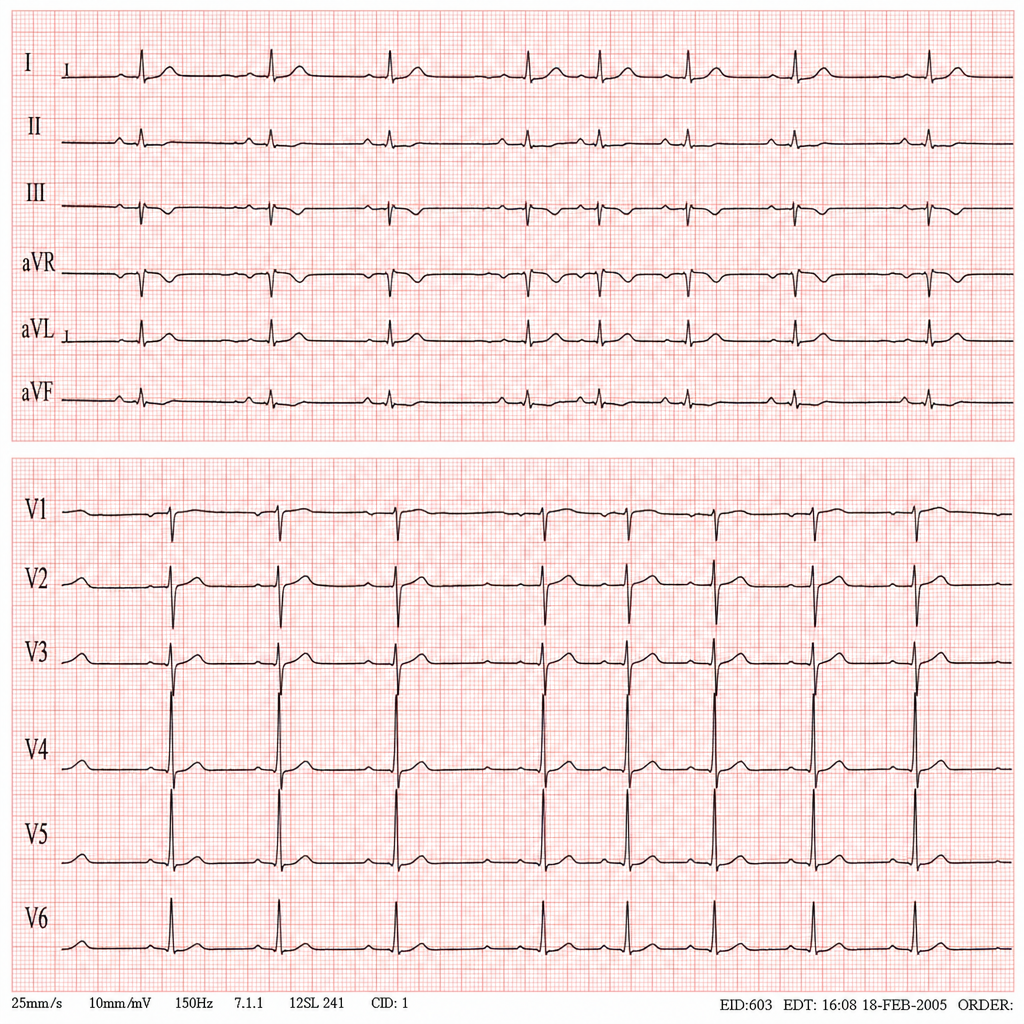
A 45-year-old man comes to the physician for a routine health maintenance examination. He feels well. He underwent appendectomy at the age of 25 years. He has a history of hypercholesterolemia that is well controlled with atorvastatin. He is an avid marathon runner and runs 8 miles per day four times a week. His father died of myocardial infarction at the age of 42 years. The patient does not smoke or drink alcohol. His vital signs are within normal limits. Cardiopulmonary examination shows no abnormalities. His abdomen is soft and nontender with a surgical scar in the right lower quadrant. Laboratory studies are within normal limits. An ECG is shown. Which of the following is the most likely diagnosis?
A 50-year-old man with a history of atrial fibrillation presents to his cardiologist’s office for a follow-up visit. He recently started treatment with an anti-arrhythmic drug to prevent future recurrences and reports that he has been feeling well and has no complaints. The physical examination shows that the arrhythmia appears to have resolved; however, there is now mild bradycardia. In addition, the electrocardiogram recording shows a slight prolongation of the PR and QT intervals. Which of the following drugs was most likely used to treat this patient?
A 70-year-old male presents for an annual exam. His past medical history is notable for shortness of breath when he sleeps, and upon exertion. Recently he has experienced dyspnea and lower extremity edema that seems to be worsening. Both of these symptoms have resolved since he was started on several medications and instructed to weigh himself daily. Which of the following is most likely a component of his medical management?
A 65-year-old man with hypertension and paroxysmal atrial fibrillation presents to his cardiologist for follow-up after recently starting metoprolol for rate control. His EKG shows an atrial rate of 260/min with ventricular rate of 50/min on an irregular baseline. An echocardiogram from his previous visit revealed no evidence of hypokinesis or hypertrophy with functionally intact valves. The patient does not drink alcohol and had no evidence of liver dysfunction in prior studies. What is the best medication for rhythm control in this patient?
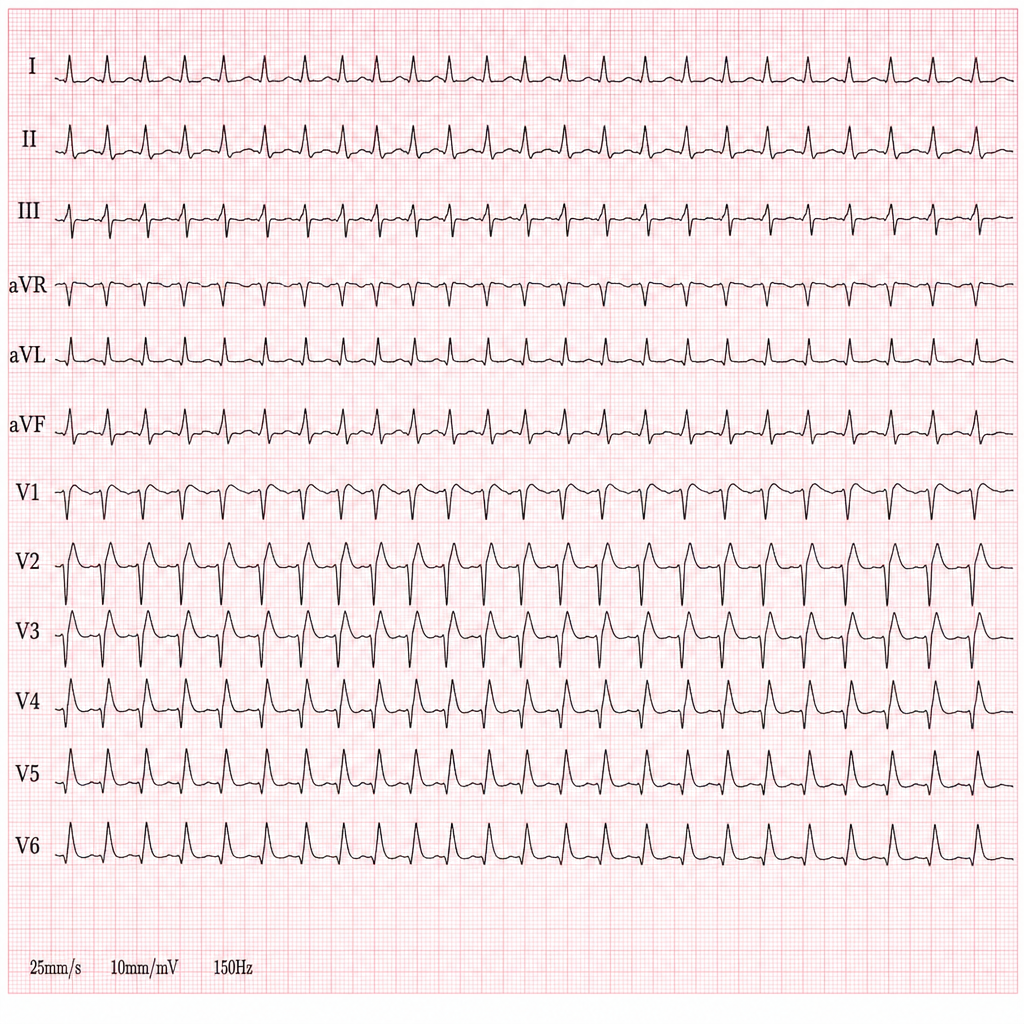
A 44-year-old woman presents with palpitations and lightheadedness. She says that symptoms onset 3 days ago and have not improved. She denies any similar episodes in this past. Her blood pressure is 140/90 mm Hg, heart rate is 150/min, respiratory rate is 16/min, and temperature is 36.6℃ (97.9℉). An ECG is performed and the results are shown in the picture. For cardioversion, it is decided to use an antiarrhythmic agent which has a use-dependent effect. Which of the following medications was most probably used?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app