
Urgent vs emergent conditions recognition — MCQs

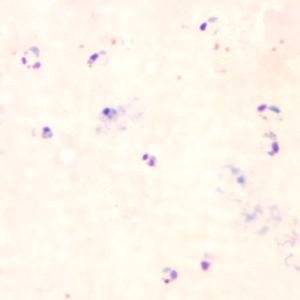
A 30-year-old woman seeks evaluation at a clinic complaining of shaking, chills, fevers, and headaches for the last 3 days. She recently returned from a trip to India, where she was visiting her family. There is no history of loss of consciousness or respiratory distress. The vital signs include temperature 38.9℃ (102.0℉), respiratory rate 19/min, blood pressure 120/80 mm Hg, and pulse 94/min (rapid and thready). On general examination, she is pale and the sclera is jaundiced. Laboratory studies show: Hematocrit (Hct) 30% Total bilirubin 2.6 mg/dL Direct bilirubin 0.3 mg/dL A peripheral smear is shown below. What is the most severe complication of this condition?
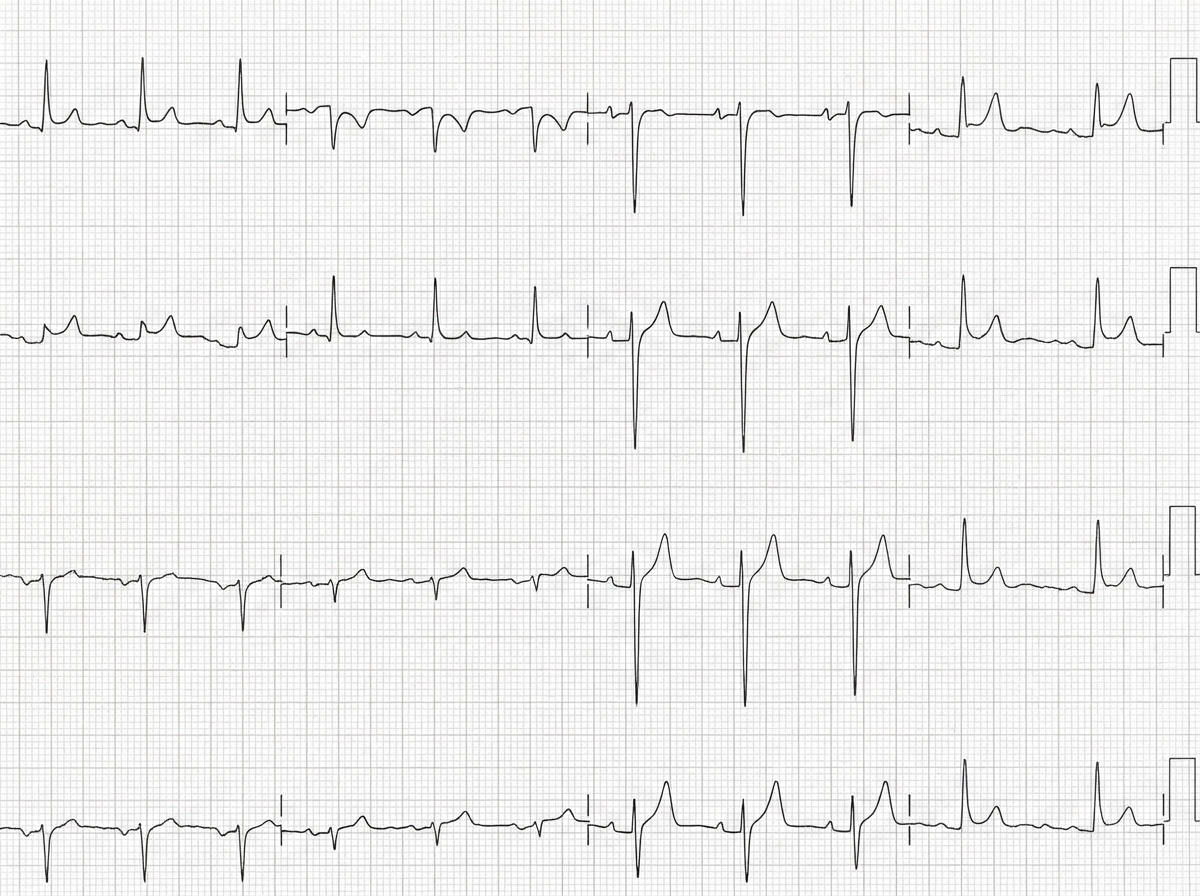
A 50-year-old man with a history of stage 4 kidney disease was admitted to the hospital for an elective hemicolectomy. His past medical history is significant for severe diverticulitis. After the procedure he becomes septic and was placed on broad spectrum antibiotics. On morning rounds, he appear weak and complains of fatigue and nausea. His words are soft and he has difficulty answering questions. His temperature is 38.9°C (102.1°F), heart rate is 110/min, respiratory rate is 15/min, blood pressure 90/65 mm Hg, and saturation is 89% on room air. On physical exam, his mental status appears altered. He has a bruise on his left arm that spontaneously appeared overnight. His cardiac exam is positive for a weak friction rub. Blood specimens are collected and sent for evaluation. An ECG is performed (see image). What therapy will this patient most likely receive next?
A 27-year-old man presents to the emergency department for altered mental status. The patient was found napping in a local market and brought to the hospital. The patient has a past medical history of polysubstance abuse and is homeless. His temperature is 104°F (40.0°C), blood pressure is 100/52 mmHg, pulse is 133/min, respirations are 25/min, and oxygen saturation is 99% on room air. Physical exam is notable for an altered man. Cardiopulmonary exam reveals a murmur over the left lower sternal border. A bedside ultrasound reveals a vegetation on the tricuspid valve. The patient is ultimately started on IV fluids, norepinephrine, vasopressin, vancomycin, and piperacillin-tazobactam. A central line is immediately placed in the internal jugular vein and the femoral vein secondary to poor IV access. Cardiothoracic surgery subsequently intervenes to remove the vegetation. While recovering in the ICU, days 3-5 are notable for an improvement in the patient’s symptoms. Two additional peripheral IVs are placed while in the ICU on day 5, and the femoral line is removed. On day 6, the patient's fever and hemodynamic status worsen. Though he is currently responding and not complaining of any symptoms including headache, photophobia, neck stiffness, or pain, he states he is feeling weak. Jolt accentuation of headache is negative and his abdominal exam is benign. A chest radiograph, urinalysis, and echocardiogram are unremarkable though the patient’s blood cultures are positive when drawn. Which of the following is the best next step in management?
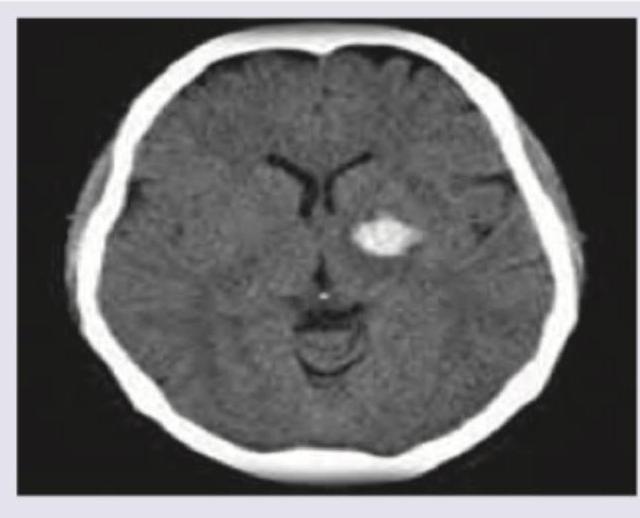
A 53-year-old man is brought to the emergency department for confusion. He was in his usual state of health until about 3 hours ago when he tried to use his sandwich to turn off the TV. He also complained to his wife that he had a severe headache. Past medical history is notable for hypertension, which has been difficult to control on multiple medications. His temperature is 36.7°C (98°F), the pulse is 70/min, and the blood pressure is 206/132 mm Hg. On physical exam he is alert and oriented only to himself, repeating over and over that his head hurts. The physical exam is otherwise unremarkable and his neurologic exam is nonfocal. The noncontrast CT scan of the patient's head is shown and reveals an acute intraparenchymal hemorrhage in the basal ganglia. Which of the following diagnostic tests would be most helpful in determining the underlying cause of this patient's hemorrhage?
A 72-year-old woman comes to the emergency department 1 hour after the sudden onset of a diffuse, dull, throbbing headache. She also reports blurred vision, nausea, and one episode of vomiting. She has a history of poorly controlled hypertension. A photograph of her fundoscopic examination is shown. Which of the following is the most likely underlying cause of this patient's symptoms?

A 57-year-old man was brought into the emergency department unconscious 2 days ago. His friends who were with him at that time say he collapsed on the street. Upon arrival to the ED, he had a generalized tonic seizure. At that time, he was intubated and is being treated with diazepam and phenytoin. A noncontrast head CT revealed hemorrhages within the pons and cerebellum with a mass effect and tonsillar herniation. Today, his blood pressure is 110/65 mm Hg, heart rate is 65/min, respiratory rate is 12/min (intubated, ventilator settings: tidal volume (TV) 600 ml, positive end-expiratory pressure (PEEP) 5 cm H2O, and FiO2 40%), and temperature is 37.0°C (98.6°F). On physical examination, the patient is in a comatose state. Pupils are 4 mm bilaterally and unresponsive to light. Cornea reflexes are absent. Gag reflex and cough reflex are also absent. Which of the following is the next best step in the management of this patient?
A 65-year-old man presents to the emergency department for sudden weakness. He was doing mechanical work on his car where he acutely developed right-leg weakness and fell to the ground. He is accompanied by his wife, who said that this has never happened before. He was last seen neurologically normal approximately 2 hours prior to presentation. His past medical history is significant for hypertension and type II diabetes. His temperature is 98.8°F (37.1°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 99% on room air. Neurological exam reveals that he is having trouble speaking and has profound weakness of his right upper and lower extremity. Which of the following is the best next step in management?
A 29-year-old man presents to the emergency department with chest pain and fatigue for the past week. The patient is homeless and his medical history is not known. His temperature is 103°F (39.4°C), blood pressure is 97/58 mmHg, pulse is 140/min, respirations are 25/min, and oxygen saturation is 95% on room air. Physical exam is notable for scars in the antecubital fossa and a murmur over the left sternal border. The patient is admitted to the intensive care unit and is treated appropriately. On day 3 of his hospital stay, the patient presents with right-sided weakness in his arm and leg and dysarthric speech. Which of the following is the most likely etiology of his current symptoms?
A 28-year-old man is admitted to the emergency department with a gunshot wound to the abdomen. He complains of weakness and diffuse abdominal pain. Morphine is administered and IV fluids are started by paramedics at the scene. On admission, the patient’s blood pressure is 90/60 mm Hg, heart rate is 103/min, respiratory rate is 17/min, the temperature is 36.2℃ (97.1℉), and oxygen saturation is 94% on room air. The patient is responsive but lethargic. The patient is diaphoretic and extremities are pale and cool. Lungs are clear to auscultation. Cardiac sounds are diminished. Abdominal examination shows a visible bullet entry wound in the left upper quadrant (LUQ) with no corresponding exit wound on the flanks or back. The abdomen is distended and diffusely tender with a rebound. Aspiration of the nasogastric tube reveals bloody contents. Rectal examination shows no blood. Stool guaiac is negative. Which of the following is the next best step in management?
A 65-year-old woman comes to the physician for the evaluation of sharp, stabbing pain in the lower back for 3 weeks. The pain radiates to the back of her right leg and is worse at night. She reports decreased sensation around her buttocks and inner thighs. During the last several days, she has had trouble urinating. Three years ago, she was diagnosed with breast cancer and was treated with lumpectomy and radiation. Her only medication is anastrozole. Her temperature is 37°C (98.6°F), pulse is 80/min, respirations are 12/min, and blood pressure is 130/70 mm Hg. Neurologic examination shows 4/5 strength in the left lower extremity and 2/5 strength in her right lower extremity. Knee and ankle reflexes are 1+ on the right. The resting anal sphincter tone is normal but the squeeze tone is reduced. Which of the following is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app