
Red flags in headache — MCQs

A 31-year-old woman presents to the emergency department with a history of fever and vomiting for 2 days and severe headache for a day. Past medical history is significant for migraine diagnosed 10 years ago, but she reports that her current headache is different. She describes the pain as generalized, dull, continuous, severe in intensity, and exacerbated by head movements. Physical examination reveals a blood pressure of 110/76 mm Hg and a temperature of 39.1°C (102.4°F). The patient is awake but in great distress due to pain. A pink-purple petechial rash covers her chest and legs. Extraocular movements are normal. She complains of neck pain and asks you to turn off the lights. Muscle strength is normal in all 4 limbs. Fundoscopic examination is normal. Baseline laboratory investigations are shown: Laboratory test Sodium 145 mEq/L Potassium 3.2 mEq/L Glucose 87 mg/dL Creatinine 1.0 mg/dL White blood cell count 18,900/mm3 Hemoglobin 13.4 g/dL Platelets 165,000/mm3 INR 1.1 Aerobic and anaerobic blood cultures are taken and empiric antibiotics are started. A lumbar puncture is performed. Which of the following cerebrospinal fluid (CSF) findings are expected in this patient?
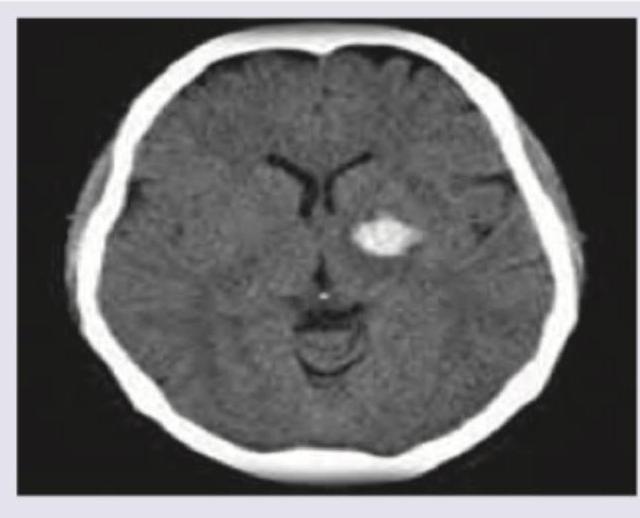
A 53-year-old man is brought to the emergency department for confusion. He was in his usual state of health until about 3 hours ago when he tried to use his sandwich to turn off the TV. He also complained to his wife that he had a severe headache. Past medical history is notable for hypertension, which has been difficult to control on multiple medications. His temperature is 36.7°C (98°F), the pulse is 70/min, and the blood pressure is 206/132 mm Hg. On physical exam he is alert and oriented only to himself, repeating over and over that his head hurts. The physical exam is otherwise unremarkable and his neurologic exam is nonfocal. The noncontrast CT scan of the patient's head is shown and reveals an acute intraparenchymal hemorrhage in the basal ganglia. Which of the following diagnostic tests would be most helpful in determining the underlying cause of this patient's hemorrhage?
A 72-year-old woman comes to the emergency department 4 hours after the sudden onset of a diffuse, dull, throbbing headache. During this time, she also reports blurred vision, nausea, and one episode of vomiting. She has a history of hypertension and type 2 diabetes mellitus. Her medications include hydrochlorothiazide, lisinopril, atorvastatin, and metformin. She has smoked 1 pack of cigarettes daily for the past 30 years and drinks 1–2 glasses of wine per day. Her temperature is 36.6 °C (97.9 °F), pulse is 90/min, respirations are 14/min, and blood pressure is 185/110 mm Hg. Fundoscopic examination shows bilateral blurring of the optic disc margins. Physical and neurologic examinations show no other abnormalities. A complete blood count and serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference range. Urinalysis shows 2+ protein but no WBCs or RBCs. Which of the following is the most likely diagnosis?
A 56-year-old woman presents with sudden-onset severe headache, nausea, vomiting, and neck pain for the past 90 minutes. She describes her headache as a ‘thunderclap’, followed quickly by severe neck pain and stiffness, nausea and vomiting. She denies any loss of consciousness, seizure, or similar symptoms in the past. Her past medical history is significant for an episode 6 months ago where she suddenly had trouble putting weight on her right leg, which resolved within hours. The patient denies any history of smoking, alcohol or recreational drug use. On physical examination, the patient has significant nuchal rigidity. Her muscle strength in the lower extremities is 4/5 on the right and 5/5 on the left. The remainder of the physical examination is unremarkable. A noncontrast CT scan of the head is normal. Which of the following is the next best step in the management of this patient?
A 62-year-old Caucasian male receiving treatment for stable angina experiences intermittent throbbing headaches. What is the most likely cause?
A 28-year-old woman presents with a 12-month history of headache, tinnitus, retrobulbar pain, and photopsias. She says the headaches are mild to moderate, intermittent, diffusely localized, and refractory to nonsteroidal anti-inflammatory drugs (NSAIDs). In addition, this past week, she began to have associated dizziness and photopsia with the headaches. Physical examination reveals a body temperature of 36.5°C (97.7°F), blood pressure of 140/80 mm Hg, and a respiratory rate of 13/min and regular. BMI is 29 kg/m2. Neurological examination is significant for peripheral visual field loss in the inferior nasal quadrant, diplopia, bilateral abducens nerve palsy, and papilledema. A T1/T2 MRI of the brain did not identify extra-axial or intra-axial masses or interstitial edema, and a lumbar puncture showed an opening pressure of 27 cm H2O, with a cerebrospinal fluid analysis within the normal range. Which of the following best describes the pathogenic mechanism underlying these findings?
A 47-year-old man presents to the clinic for an evaluation of intense itching of his right thigh region for the past few days. He states some ‘red bumps’ just began to form. The patient mentions that he was recently at a business conference in Miami. He has a past medical history of hypertension, diabetes type 2, and hyperlipidemia. He takes enalapril, metformin, and atorvastatin. He does not smoke or drink. His vitals are within normal limits today. On physical examination, a linear line with 3 red papules is present along the medial aspect of his right thigh. Additionally, there are small rows of bumps on his left leg and right forearm. Excoriations are also apparent in the same region. Which of the following is the most likely diagnosis?
A 67-year-old man with type 2 diabetes mellitus and benign prostatic hyperplasia comes to the physician because of a 2-day history of sneezing and clear nasal discharge. He has had similar symptoms occasionally in the past. His current medications include metformin and tamsulosin. Examination of the nasal cavity shows red, swollen turbinates. Which of the following is the most appropriate pharmacotherapy for this patient's condition?
A 31-year-old man and his wife were referred to a genetic counselor. They are concerned about the chance that their children are likely to inherit certain conditions that run in their families. The wife's father and grandfather are both healthy, but her grandfather cannot see the color red. The husband is unaware if any member of his family has the same condition. The geneticist provides some details about genetic diseases and inheritance patterns, then orders lab tests to analyze the gene mutations carried by both partners. Which of the following are the correct terms regarding the genotype and phenotype of males affected by the condition described?
A 43-year-old woman was admitted to the hospital after a fall. When the emergency services arrived, she was unresponsive, did not open her eyes, but responded to painful stimuli. The witnesses say that she had convulsions lasting about 30 seconds when she lost consciousness after a traumatic event. On her way to the hospital, she regained consciousness. On admission, she complained of intense headaches and nausea. She opened her eyes spontaneously, was responsive but confused, and was able to follow motor commands. Her vital signs are as follows: blood pressure, 150/90 mm Hg; heart rate, 62/min; respiratory rate, 13/min; and temperature, 37.3℃ (99.1℉). There are no signs of a skull fracture. The pupils are round, equal, and poorly reactive to light. She is unable to fully abduct both eyes. Ophthalmoscopy does not show papillary edema or retinal hemorrhages. She has nuchal rigidity and a positive Kernig sign. An urgent head CT does not show any abnormalities. Which of the following is a proper investigation to perform in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app