
Red flags in dyspnea — MCQs

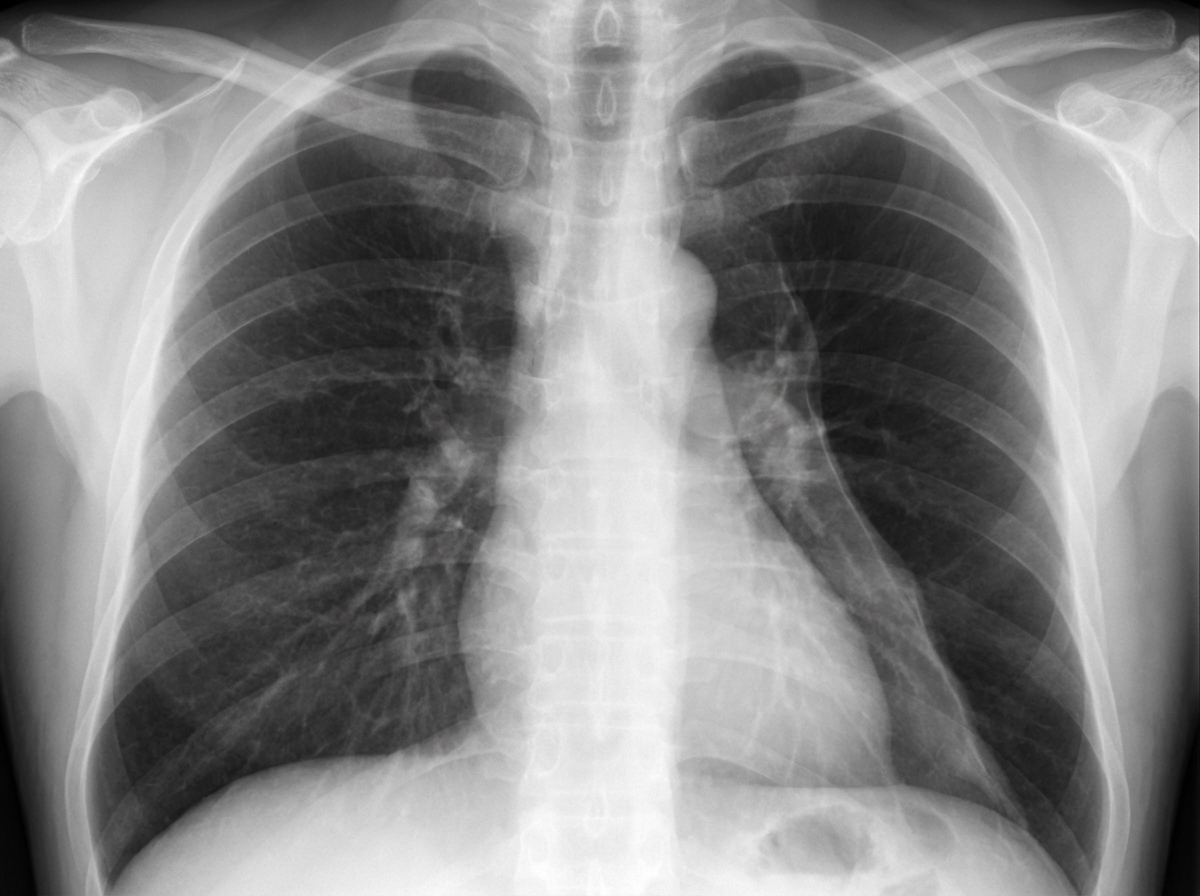
A 19-year-old man comes to the emergency department with sharp, left-sided chest pain and shortness of breath. He has no history of recent trauma. He does not smoke or use illicit drugs. He is 196 cm (6 feet 5 in) tall and weighs 70 kg (154 lb); BMI is 18 kg/m2. Examination shows reduced breath sounds over the left lung field. An x-ray of the chest is shown. Which of the following changes is most likely to immediately result from this patient's current condition?
A 36-year-old man presents to the physician with difficulty in breathing for 3 hours. There is no history of chest pain, cough or palpitation. He is a chronic smoker and underwent elective cholecystectomy one month back. There is no history of chronic or recurrent cough, wheezing or breathlessness. His temperature is 38.2°C (100.8°F), pulse is 108/min, blood pressure is 124/80 mm Hg, and respirations are 25/min. His arterial oxygen saturation is 98% in room air as shown by pulse oximetry. After a detailed physical examination, the physician orders a plasma D-dimer level, which was elevated. A contrast-enhanced computed tomography (CT) of the chest shows a filling defect in a segmental pulmonary artery on the left side. Which of the following signs is most likely to have been observed by the physician during the physical examination of this patient’s chest?
A previously healthy 21-year-old man is brought to the emergency department 4 hours after the sudden onset of shortness of breath and pleuritic chest pain. He has smoked 1 pack of cigarettes daily for the past 3 years. He is 188 cm (6.2 ft) tall and weighs 70 kg (154 lb); BMI is 19.8 kg/m2. Physical examination shows decreased tactile fremitus and diminished breath sounds over the left lung. Which of the following is the most likely cause of this patient's symptoms?
A 55-year-old man is brought to the emergency department 30 minutes after the sudden onset of severe, migrating anterior chest pain, shortness of breath, and sweating at rest. He has hypertension, hypercholesterolemia, and type 2 diabetes mellitus. Medications include atorvastatin, hydrochlorothiazide, lisinopril, and metformin. He has smoked one pack of cigarettes daily for 25 years. He is in severe distress. His pulse is 110/min, respirations are 20/min, and blood pressure is 150/85 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. Cardiac examination shows a grade 3/6, high-pitched, blowing, diastolic murmur heard best over the right sternal border. The lungs are clear to auscultation. Femoral pulses are decreased bilaterally. An ECG shows sinus tachycardia and left ventricular hypertrophy. Which of the following is the most likely diagnosis?
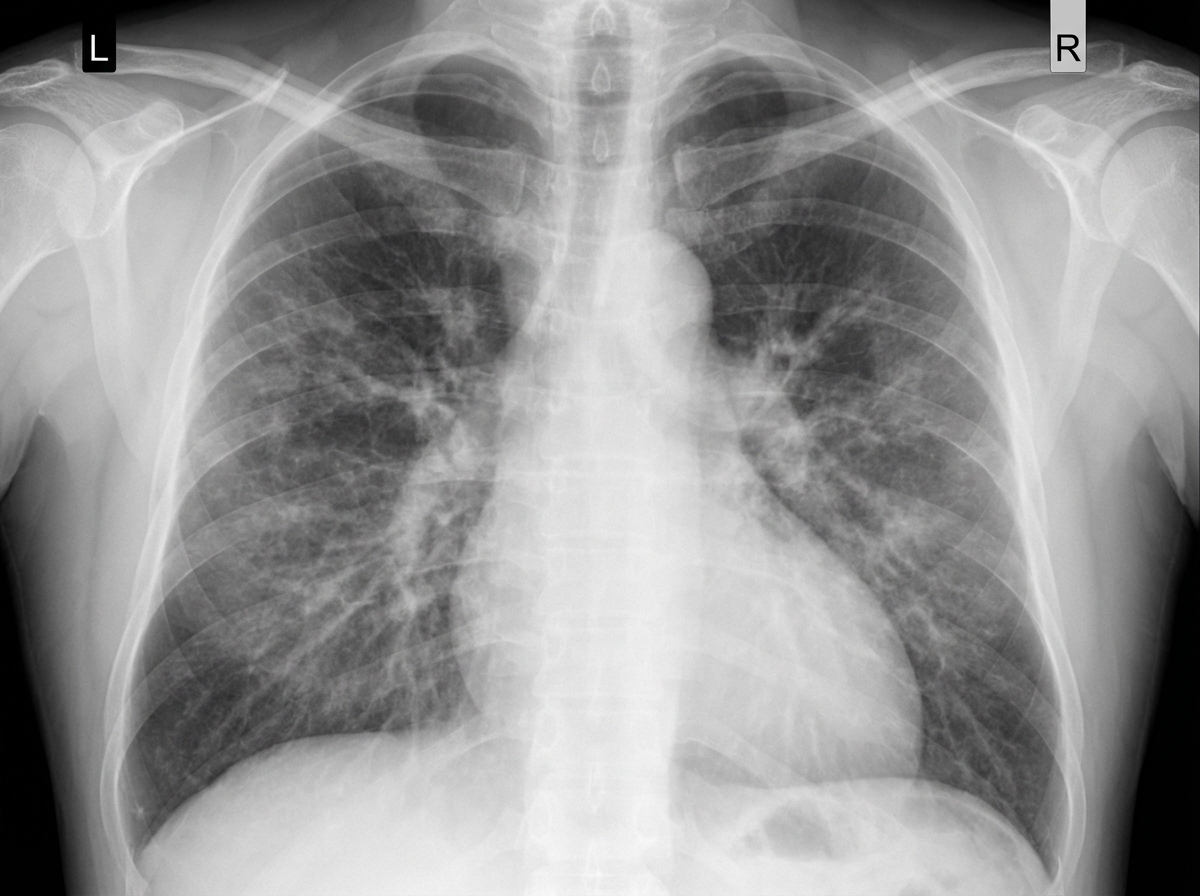
A 58-year-old man comes to the physician because of a 5-day history of progressively worsening shortness of breath and fatigue. He has smoked 1 pack of cigarettes daily for 30 years. His pulse is 96/min, respirations are 26/min, and blood pressure is 100/60 mm Hg. An x-ray of the chest is shown. Which of the following is the most likely cause of this patient's findings?
A 21-year-old man presents with fever, headache, and clouded sensorium for the past 3 days. His fever is low-grade. He says his headache is mild-to-moderate in intensity and associated with nausea, vomiting, and photophobia. There is no history of a sore throat, pain on urination, abdominal pain, or loose motions. He smokes 1–2 cigarettes daily and drinks alcohol socially. Past medical history and family history are unremarkable. His vital signs include: blood pressure 120/80 mm Hg, pulse 106/min, temperature 37.3°C (99.2°F). On physical examination, he is confused, disoriented, and agitated. Extraocular movements are intact. The neck is supple on flexion. He is moving all his 4 limbs spontaneously. A noncontrast CT scan of the head is within normal limits. A lumbar puncture is performed, and cerebrospinal fluid results are still pending. The patient is started on empiric intravenous acyclovir. Which of the following clinical features favors encephalitis rather than meningitis?
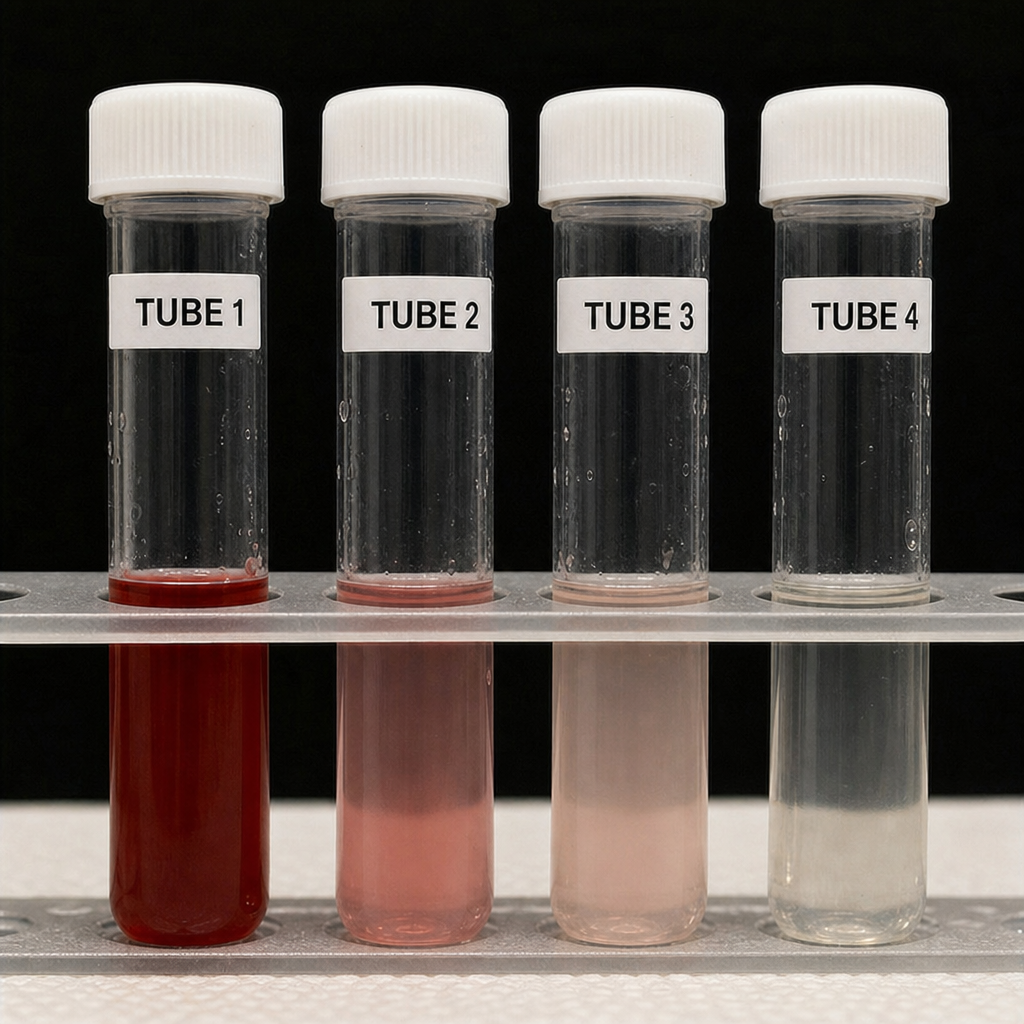
A 29-year-old man presents to the emergency department with sudden onset of the worst headache of his life that began 45 minutes ago while lifting weights. He rates the pain 10/10 and describes it as 'like being hit in the back of the head.' He vomited once. Temperature is 37.2°C, blood pressure 148/90 mmHg, heart rate 98 bpm. Neurological examination is intact; there is no papilledema and no meningismus. Non-contrast CT of the head is performed and reported as normal. The image shown is the lumbar puncture result obtained 12 hours after symptom onset. Based on the image findings and clinical context, what is the most appropriate interpretation of this diagnostic result?
A 55-year-old woman with a 6-month history of progressive exertional dyspnea and bilateral leg swelling presents to the clinic. She has no history of smoking, cardiac disease, or prior lung disease. She takes no medications. Vitals: BP 118/74 mmHg, HR 96 bpm, SpO₂ 91% on room air. Exam reveals elevated JVP, a loud P2, and pitting edema to the knees. A chest radiograph is obtained and shows enlarged central pulmonary arteries with peripheral pruning, a prominent right heart border, and no evidence of pulmonary venous congestion or interstitial edema. Based on the clinical and radiographic findings, which of the following is the most likely underlying diagnosis?

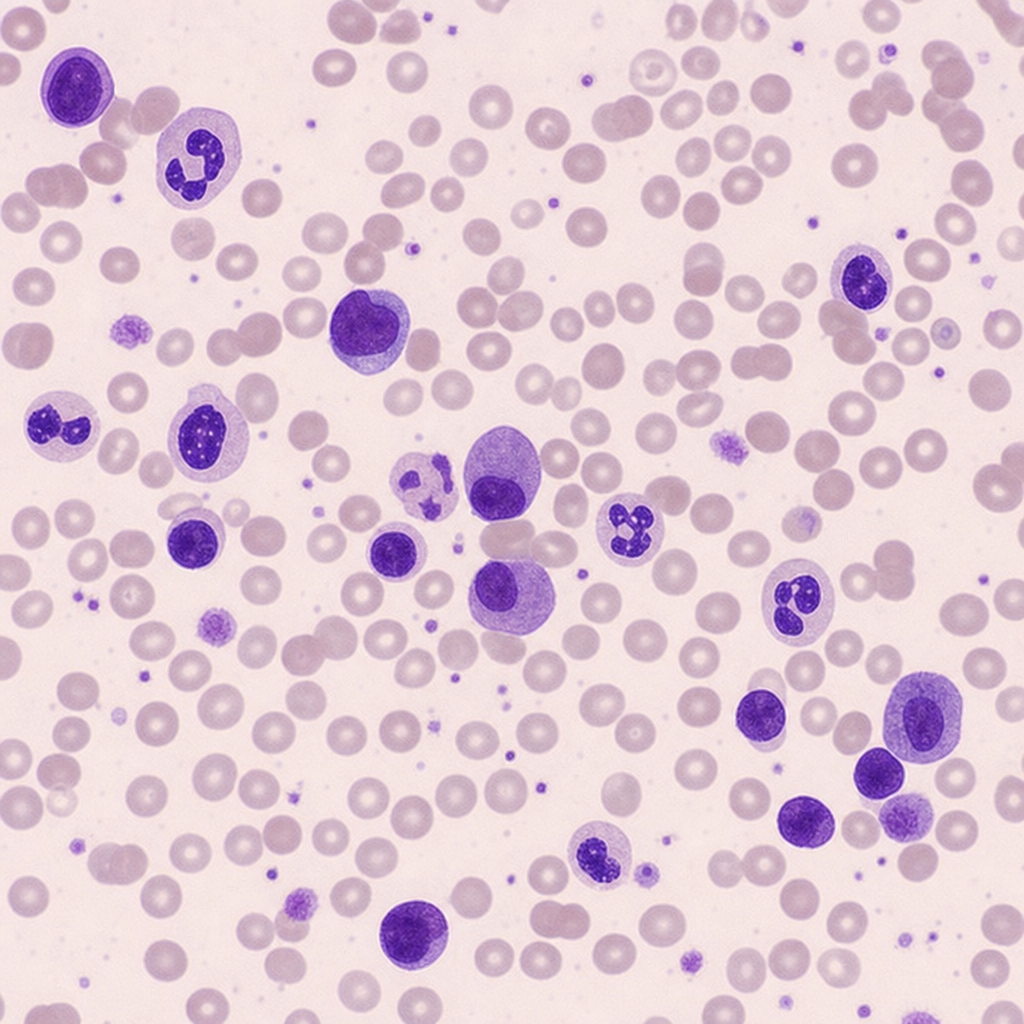
A 61-year-old woman is referred for evaluation of a 5-month history of progressive fatigue, 8-kg unintentional weight loss, and new-onset low back pain. She has no prior malignancy and takes no medications. Physical examination reveals mild pallor and point tenderness over the lumbar spine at L3–L4. Laboratory studies: hemoglobin 9.1 g/dL (MCV 88 fL), serum calcium 11.4 mg/dL, creatinine 1.9 mg/dL, total protein 10.2 g/dL, albumin 3.8 g/dL. A peripheral blood smear is shown. The finding on the smear, integrated with the full clinical picture, most strongly supports which diagnosis?
A 3-year-old boy is brought to the emergency department with fever, irritability, and refusal to walk for 12 hours. His parents report he had a fall 3 days ago but seemed fine afterward. Temperature is 39.2°C (102.5°F), pulse 140/min. He cries when his right hip is moved and holds it in flexion and external rotation. WBC is 18,000/μL, ESR 65 mm/hr, CRP 8.5 mg/dL. He appears ill and has not responded to acetaminophen. Apply clinical reasoning to determine the most appropriate next step.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app