
Red flags — MCQs

On this page
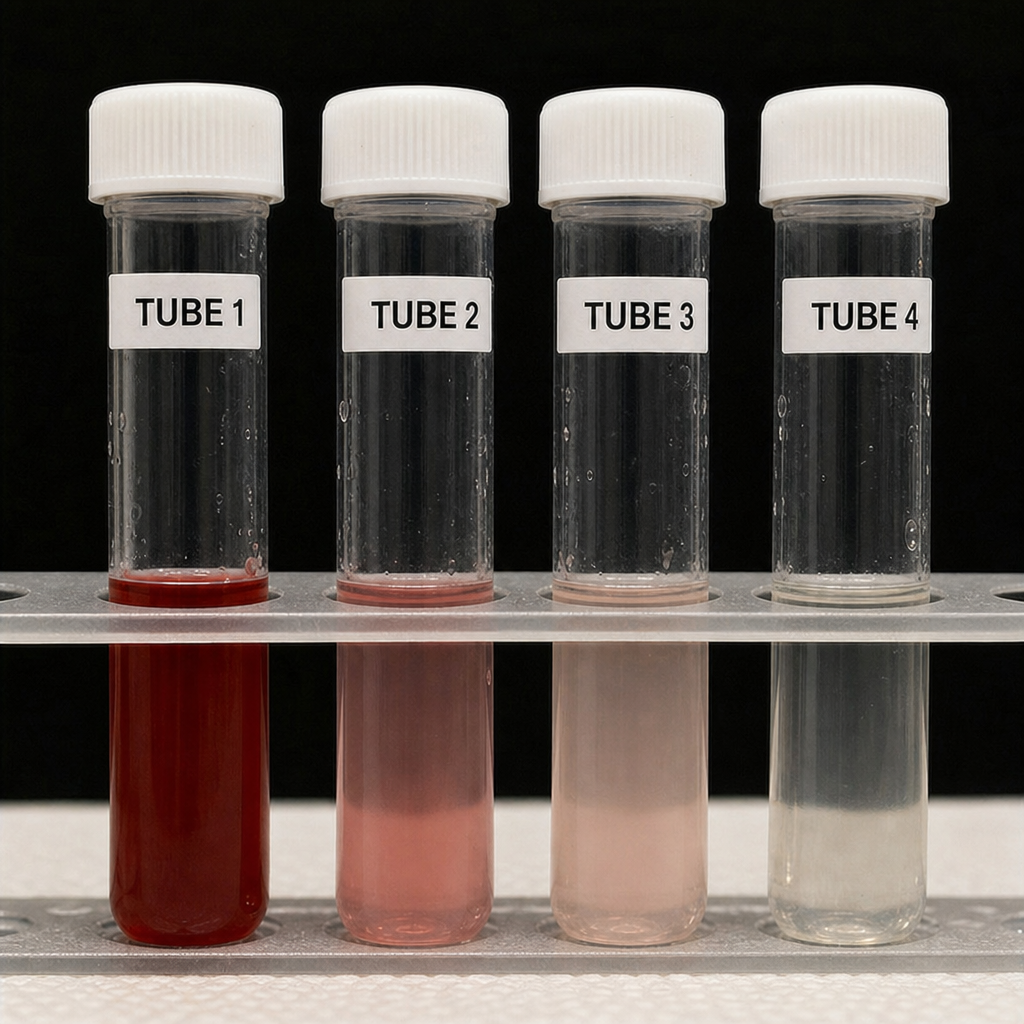
A 29-year-old man presents to the emergency department with sudden onset of the worst headache of his life that began 45 minutes ago while lifting weights. He rates the pain 10/10 and describes it as 'like being hit in the back of the head.' He vomited once. Temperature is 37.2°C, blood pressure 148/90 mmHg, heart rate 98 bpm. Neurological examination is intact; there is no papilledema and no meningismus. Non-contrast CT of the head is performed and reported as normal. The image shown is the lumbar puncture result obtained 12 hours after symptom onset. Based on the image findings and clinical context, what is the most appropriate interpretation of this diagnostic result?
A 55-year-old woman with a 6-month history of progressive exertional dyspnea and bilateral leg swelling presents to the clinic. She has no history of smoking, cardiac disease, or prior lung disease. She takes no medications. Vitals: BP 118/74 mmHg, HR 96 bpm, SpO₂ 91% on room air. Exam reveals elevated JVP, a loud P2, and pitting edema to the knees. A chest radiograph is obtained and shows enlarged central pulmonary arteries with peripheral pruning, a prominent right heart border, and no evidence of pulmonary venous congestion or interstitial edema. Based on the clinical and radiographic findings, which of the following is the most likely underlying diagnosis?

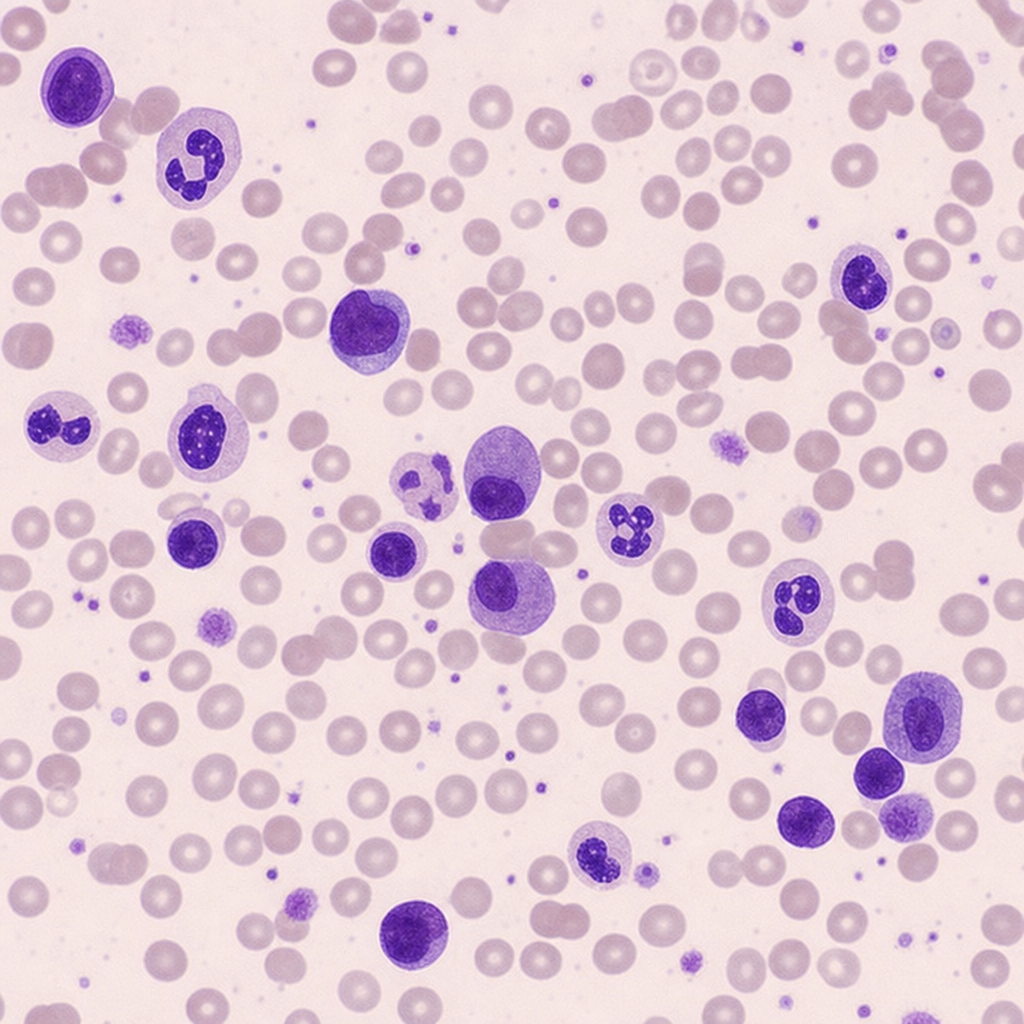
A 61-year-old woman is referred for evaluation of a 5-month history of progressive fatigue, 8-kg unintentional weight loss, and new-onset low back pain. She has no prior malignancy and takes no medications. Physical examination reveals mild pallor and point tenderness over the lumbar spine at L3–L4. Laboratory studies: hemoglobin 9.1 g/dL (MCV 88 fL), serum calcium 11.4 mg/dL, creatinine 1.9 mg/dL, total protein 10.2 g/dL, albumin 3.8 g/dL. A peripheral blood smear is shown. The finding on the smear, integrated with the full clinical picture, most strongly supports which diagnosis?
A 3-year-old boy is brought to the emergency department with fever, irritability, and refusal to walk for 12 hours. His parents report he had a fall 3 days ago but seemed fine afterward. Temperature is 39.2°C (102.5°F), pulse 140/min. He cries when his right hip is moved and holds it in flexion and external rotation. WBC is 18,000/μL, ESR 65 mm/hr, CRP 8.5 mg/dL. He appears ill and has not responded to acetaminophen. Apply clinical reasoning to determine the most appropriate next step.
A 25-year-old previously healthy woman presents with 3 days of severe diffuse abdominal pain, vomiting, and dark urine. She recently started a low-carbohydrate diet for weight loss. She appears anxious and confused. Vital signs show BP 145/95 mmHg, pulse 110/min. Examination reveals diffuse abdominal tenderness without peritoneal signs. Labs show sodium 128 mEq/L, normal white blood cell count, and urine is dark red but dipstick negative for blood. She has new-onset weakness in her upper extremities. Synthesize these findings to determine the underlying diagnosis and management approach.
Practice by Chapter
Red flags in neurological complaints
Practice Questions
Red flags in chest pain
Practice Questions
Red flags in abdominal pain
Practice Questions
Red flags in pediatric presentations
Practice Questions
Red flags in geriatric patients
Practice Questions
Red flags in mental health assessment
Practice Questions
Red flags in musculoskeletal complaints
Practice Questions
Red flags in headache
Practice Questions
Red flags in fever
Practice Questions
Red flags in dyspnea
Practice Questions
Red flags in skin conditions
Practice Questions
Red flags in pregnancy
Practice Questions
Urgent vs emergent conditions recognition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app