
Differential diagnosis — MCQs

On this page
A 33-year-old man presents to his primary care physician for left-sided knee pain. The patient has a history of osteoarthritis but states that he has been unable to control his pain with escalating doses of ibuprofen and naproxen. His past medical history includes diabetes mellitus and hypertension. His temperature is 102.0°F (38.9°C), blood pressure is 167/108 mmHg, pulse is 100/min, respirations are 14/min, and oxygen saturation is 98% on room air. Physical exam reveals a warm and tender joint that is very tender to the touch and with passive range of motion. The patient declines a gait examination secondary to pain. Which of the following is the best next step in management?
A 23-year-old woman presents with a painful lesion in her mouth. She denies tooth pain, bleeding from the gums, nausea, vomiting, diarrhea, or previous episodes similar to this in the past. She states that her last normal menstrual period was 12 days ago, and she has not been sexually active since starting medical school 2 years ago. On physical examination, the patient has good dentition with no signs of infection with the exception of a solitary ulcerated lesion on the oral mucosa. The nonvesicular lesion has a clean gray-white base and is surrounded by erythema. Which of the following is correct concerning the most likely etiology of the oral lesion in this patient?
A 19-year-old girl comes to her physician with blurred vision upon awakening for 3 months. When she wakes up in the morning, both eyelids are irritated, sore, and covered with a dry crust. Her symptoms improve after she takes a hot shower. She is otherwise healthy and takes no medications. She does not wear contact lenses. Recently, she became sexually active with a new male partner. Her temperature is 37.4°C (99.3°F), and pulse is 88/minute. Both eyes show erythema and irritation at the superior lid margin, and there are flakes at the base of the lashes. There is no discharge. Visual acuity is 20/20 bilaterally. Which of the following is the next best step in management?
A 43-year-old man comes to the physician for a follow-up examination. Four months ago, he was treated conservatively for ureteric colic. He has noticed during micturition that his urine is reddish-brown initially and then clears by the end of the stream. He has no dysuria. He has hypertension. His only medication is hydrochlorothiazide. He appears healthy and well-nourished. His temperature is 37°C (98.6°F), pulse is 80/min, and blood pressure is 122/86 mm Hg. Physical examination shows no abnormalities. Laboratory studies show: Hemoglobin 14.1 g/dL Serum Glucose 88 mg/dL Creatinine 0.6 mg/dL Urine Blood 2+ Protein negative Leukocyte esterase negative Nitrite negative RBCs 5–7/hpf WBCs 0–1/hpf RBC casts none Which of the following is the most likely origin of this patient's hematuria?
A 24-year-old woman presents to the emergency department for chest pain and shortness of breath. She was at home making breakfast when her symptoms began. She describes the pain as sharp and located in her chest. She thought she was having a heart attack and began to feel short of breath shortly after. The patient is a college student and recently joined the soccer team. She has no significant past medical history except for a progesterone intrauterine device which she uses for contraception, and a cyst in her breast detected on ultrasound. Last week she returned on a trans-Atlantic flight from Russia. Her temperature is 98.4°F (36.9°C), blood pressure is 137/69 mmHg, pulse is 98/min, respirations are 18/min, and oxygen saturation is 99% on room air. Physical exam reveals an anxious young woman. Cardiac and pulmonary exam are within normal limits. Deep inspiration and palpation of the chest wall elicits pain. Neurologic exam reveals a stable gait and cranial nerves II-XII are grossly intact. Which of the following best describes the most likely underlying etiology?
A 41-year-old woman with a past medical history significant for asthma and seasonal allergies presents with a new rash. She has no significant past surgical, social, or family history. The patient's blood pressure is 131/90 mm Hg, the pulse is 77/min, the respiratory rate is 17/min, and the temperature is 36.9°C (98.5°F). Physical examination reveals a sharply demarcated area of skin dryness and erythema encircling her left wrist. Review of systems is otherwise negative. Which of the following is the most likely diagnosis?
A previously healthy 33-year-old woman comes to the physician because of pain and sometimes numbness in her right thigh for the past 2 months. She reports that her symptoms are worse when walking or standing and are better while sitting. Three months ago, she started going to a fitness class a couple times a week. She is 163 cm (5 ft 4 in) tall and weighs 88 kg (194 lb); BMI is 33.1 kg/m2. Her vital signs are within normal limits. Examination of the skin shows no abnormalities. Sensation to light touch is decreased over the lateral aspect of the right anterior thigh. Muscle strength is normal. Tapping the right inguinal ligament leads to increased numbness of the affected thigh. The straight leg test is negative. Which of the following is the most appropriate next step in management of this patient?
Nine days after being treated for a perforated gastric ulcer and sepsis, a 78-year-old woman develops decreased urinary output and malaise. She required emergency laparotomy and was subsequently treated in the intensive care unit for sepsis. Blood cultures grew Pseudomonas aeruginosa. The patient was treated with ceftazidime and gentamicin. She has type 2 diabetes mellitus, arterial hypertension, and osteoarthritis of the hips. Prior to admission, her medications were insulin, ramipril, and ibuprofen. Her temperature is 37.3°C (99.1°F), pulse is 80/min, and blood pressure is 115/75 mm Hg. Examination shows a healing surgical incision in the upper abdomen. Laboratory studies show: Hemoglobin count 14 g/dL Leukocyte count 16,400 mm3 Segmented neutrophils 60% Eosinophils 2% Lymphocytes 30% Monocytes 6% Platelet count 260,000 mm3 Serum Na+ 137 mEq/L Cl- 102 mEq/L K+ 5.1 mEq/L Urea nitrogen 25 mg/dL Creatinine 4.2 mg/dL Fractional excretion of sodium is 2.1%. Which of the following findings on urinalysis is most likely associated with this patient's condition?
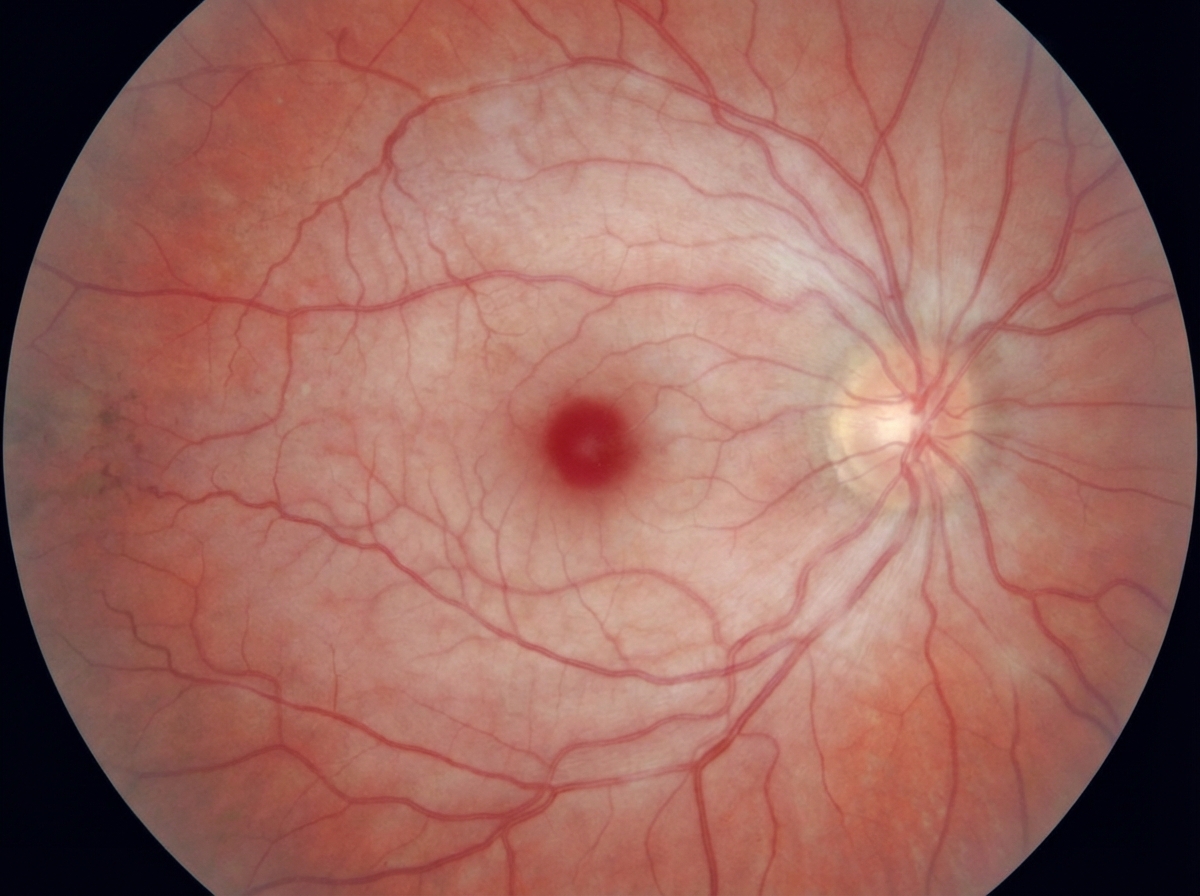
A 65-year-old man presents to the emergency department because of a sudden loss of vision in his left eye for 2 hours. He has no pain. He had a similar episode 1 month ago which lasted only seconds. He has no history of a headache or musculoskeletal pain. He has had ischemic heart disease for 8 years and hypertension and diabetes mellitus for 13 years. His medications include metoprolol, aspirin, insulin, lisinopril, and atorvastatin. He has smoked 1 pack of cigarettes for 39 years. The vital signs include: blood pressure 145/98 mm Hg, pulse 86/min, respirations 16/min, and temperature 36.7°C (98.1°F). Physical examination of the left eye shows a loss of light perception. After illumination of the right eye and consensual constriction of the pupils, illumination of the left eye shows pupillary dilation. A fundoscopy image is shown. Which of the following best explains these findings?
A 19-year-old woman undergoes a laparoscopic appendectomy for acute appendicitis. During the procedure, a black, discolored liver is noted. Other than the recent appendicitis, the patient has no history of serious illness and takes no medications. She has no medication allergies. She does not drink alcohol or use illicit drugs. She has an uncomplicated postoperative course. At her follow-up visit 3 weeks later, her vital signs are within normal limits. Examination shows scleral icterus, which the patient states has been present for many years. Abdominal examination shows healing scars without drainage or erythema. Serum studies show: Aspartate aminotransferase 30 IU/L Alanine aminotransferase 35 IU/L Alkaline phosphatase 47 IU/L Total bilirubin 5.2 mg/dL Direct bilirubin 4.0 mg/dL Which of the following is the most likely diagnosis?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app