
Differential diagnosis — MCQs

On this page
A 67-year-old man presents with pain in both legs. He says the pain is intermittent in nature and has been present for approximately 6 months. The pain increases with walking, especially downhill, and prolonged standing. It is relieved by lying down and leaning forward. Past medical history is significant for type 2 diabetes mellitus, hypercholesterolemia, and osteoarthritis. The patient reports a 56-pack-year history but denies any alcohol or recreational drug use. His vital signs include: blood pressure 142/88 mm Hg, pulse 88/min, respiratory rate 14/min, temperature 37°C (98.6°F). On physical examination, the patient is alert and oriented. Muscle strength is 5/5 in his upper and lower extremities bilaterally. Babinski and Romberg tests are negative. Pulses measure 2+ in upper and lower extremities bilaterally. Which of the following is the next best step in the management of this patient?
A 55-year-old man presents to the emergency department with fatigue and a change in his memory. The patient and his wife state that over the past several weeks the patient has been more confused and irritable and has had trouble focusing. He has had generalized and non-specific pain in his muscles and joints and is constipated. His temperature is 99.3°F (37.4°C), blood pressure is 172/99 mmHg, pulse is 79/min, respirations are 14/min, and oxygen saturation is 99% on room air. Physical exam is unremarkable. Laboratory studies are ordered as seen below. Hemoglobin: 9.0 g/dL Hematocrit: 30% Leukocyte count: 6,500/mm^3 with normal differential Platelet count: 166,000/mm^3 MCV: 78 fL Serum: Na+: 141 mEq/L Cl-: 103 mEq/L K+: 4.6 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 0.9 mg/dL Ca2+: 10.2 mg/dL Which of the following is the most likely diagnosis?
A 37-year-old man comes to the physician because of increasing swelling and pain of his right knee for the past month. He has not had any trauma to the knee or previous problems with his joints. He has hypertension. His only medication is hydrochlorothiazide. He works as a carpet installer. He drinks two to three beers daily. He is 170 cm (5 ft 7 in) tall and weighs 97 kg (214 lb); BMI is 33.6 kg/m2. His temperature is 37°C (98.6°F), pulse is 88/min, and blood pressure is 122/82 mm Hg. Examination of the right knee shows swelling and erythema; there is fluctuant edema over the lower part of the patella. The range of flexion is limited because of the pain. The skin over the site of his pain is not warm. There is tenderness on palpation of the patella; there is no joint line tenderness. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?
A 65-year-old woman comes to the physician for the evaluation of sharp, stabbing pain in the lower back for 3 weeks. The pain radiates to the back of her right leg and is worse at night. She reports decreased sensation around her buttocks and inner thighs. During the last several days, she has had trouble urinating. Three years ago, she was diagnosed with breast cancer and was treated with lumpectomy and radiation. Her only medication is anastrozole. Her temperature is 37°C (98.6°F), pulse is 80/min, respirations are 12/min, and blood pressure is 130/70 mm Hg. Neurologic examination shows 4/5 strength in the left lower extremity and 2/5 strength in her right lower extremity. Knee and ankle reflexes are 1+ on the right. The resting anal sphincter tone is normal but the squeeze tone is reduced. Which of the following is the most likely diagnosis?
A 35-year-old male presents to his primary care physician with pain along the bottom of his foot. The patient is a long-time runner but states that the pain has been getting worse recently. He states that when running and at rest he has a burning and aching pain along the bottom of his foot that sometimes turns to numbness. Taking time off from training does not improve his symptoms. The patient has a past medical history of surgical repair of his Achilles tendon, ACL, and medial meniscus. He is currently not taking any medications. The patient lives with his wife and they both practice a vegan lifestyle. On physical exam the patient states that he is currently not experiencing any pain in his foot but rather is experiencing numbness/tingling along the plantar surface of his foot. Strength is 5/5 and reflexes are 2+ in the lower extremities. Which of the following is the most likely diagnosis?
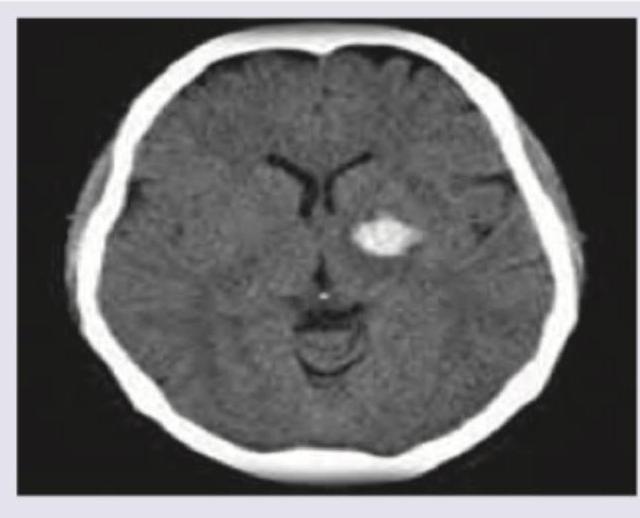
A 53-year-old man is brought to the emergency department for confusion. He was in his usual state of health until about 3 hours ago when he tried to use his sandwich to turn off the TV. He also complained to his wife that he had a severe headache. Past medical history is notable for hypertension, which has been difficult to control on multiple medications. His temperature is 36.7°C (98°F), the pulse is 70/min, and the blood pressure is 206/132 mm Hg. On physical exam he is alert and oriented only to himself, repeating over and over that his head hurts. The physical exam is otherwise unremarkable and his neurologic exam is nonfocal. The noncontrast CT scan of the patient's head is shown and reveals an acute intraparenchymal hemorrhage in the basal ganglia. Which of the following diagnostic tests would be most helpful in excluding an underlying macrovascular lesion as the cause of this patient's hemorrhage?
A 29-year-old woman comes to the physician because of a 2-day history of intermittent dark urine and mild flank pain. She has also had a cough, sore throat, and runny nose for the past 5 days. She has not had dysuria. She takes no medications. She has no known allergies. Her temperature is 37°C (98.6°F). Examination of the back shows no costovertebral angle tenderness. Laboratory studies show: Hemoglobin 10.4 g/dL Leukocyte count 8,000/mm3 Platelet count 200,000/mm3 Serum Na+ 135 mEq/L K+ 4.9 mEq/L Cl- 101 mEq/L HCO3- 22 mEq/L Urea nitrogen 18 mg/dL Creatinine 1.1 mg/dL Urine Color yellow Blood 3+ Protein 1+ Leukocyte esterase negative An ultrasound of the kidney and bladder shows no abnormalities. Which of the following is the most likely cause of this patient's symptoms?
A 45-year-old woman presents to her primary care physician for knee pain. She states that she has been experiencing a discomfort and pain in her left knee that lasts for several hours but tends to improve with use. She takes ibuprofen occasionally which has been minimally helpful. She states that this pain is making it difficult for her to work as a cashier. Her temperature is 98.6°F (37.0°C), blood pressure is 117/58 mmHg, pulse is 90/min, respirations are 14/min, and oxygen saturation is 97% on room air. Physical exam reveals a stable gait that the patient claims causes her pain. The patient has a non-pulsatile, non-erythematous, palpable mass over the posterior aspect of her left knee that is roughly 3 to 4 cm in diameter and is hypoechoic on ultrasound. Which of the following is associated with this patient's condition?
A 43-year-old woman presents to the neurology clinic in significant pain. She reports a sharp, stabbing electric-like pain on the right side of her face. The pain started suddenly 2 weeks ago. The pain is so excruciating that she can no longer laugh, speak, or eat her meals as these activities cause episodes of pain. She had to miss work last week as a result. Her attacks last about 3 minutes and go away when she goes to sleep. She typically has 2–3 attacks per day now. The vital signs include: blood pressure 132/84 mm Hg, heart rate 79/min, and respiratory rate 14/min. A neurological examination shows no loss of crude touch, tactile touch, or pain sensations on the right side of the face. The pupillary light and accommodation reflexes are normal. There is no drooping of her mouth, ptosis, or anhidrosis noted. Which of the following is the most likely diagnosis?
A 60-year-old male is admitted to the ICU for severe hypertension complicated by a headache. The patient has a past medical history of insulin-controlled diabetes, hypertension, and hyperlipidemia. He smokes 2 packs of cigarettes per day. He states that he forgot to take his medications yesterday and started getting a headache about one hour ago. His vitals on admission are the following: blood pressure of 160/110 mmHg, pulse 95/min, temperature 98.6 deg F (37.2 deg C), and respirations 20/min. On exam, the patient has an audible abdominal bruit. After administration of antihypertensive medications, the patient has a blood pressure of 178/120 mmHg. The patient reports his headache has increased to a 10/10 pain level, that he has trouble seeing, and he can't move his extremities. After stabilizing the patient, what is the best next step to diagnose the patient's condition?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app