
Differential diagnosis — MCQs

On this page
Three days after undergoing laparoscopic colectomy, a 67-year-old man reports swelling and pain in his right leg. He was diagnosed with colon cancer 1 month ago. His temperature is 38.5°C (101.3°F). Physical examination shows swelling of the right leg from the ankle to the thigh. There is no erythema or rash. Which of the following is likely to be most helpful in establishing the diagnosis?
A 52-year-old woman with type 2 diabetes mellitus comes to the physician because of a 2-day history of blisters on her forearms and pain during sexual intercourse. Her only medications are metformin and glyburide. Examination reveals multiple, flaccid blisters on the volar surface of the forearms and ulcers on the buccal, gingival, and vulvar mucosa. The epidermis on the forearm separates when the skin is lightly stroked. Which of the following is the most likely diagnosis?
A 65-year-old woman presents to a dermatology clinic complaining about numerous well-demarcated, dark, round skin lesions on her face and back. She claims she has had these lesions for 3 or 4 years. The lesions are painless, not pruritic, and have never bled. However, she is moderately distressed about the potential malignancy of these lesions after she heard that a close friend was just diagnosed with a melanoma. The medical history is unremarkable. Physical examination reveals numerous well-demarcated, round, verrucous lesions, with a stuck-on appearance, distributed on the patient's back and face (see image). Under a dermatoscope, the lesions showed multiple comedo-like openings, milia cysts, and a cerebriform pattern. What is the best next step of management?

A 32-year-old man comes to the emergency department for acute pain in the left eye. He reports having awoken in the morning with a foreign body sensation. He had forgotten to remove his contact lenses before sleeping. Following lens removal, he experienced immediate pain, discomfort, and tearing of the left eye. He reports that the foreign body sensation persists and that rinsing with water has not improved the pain. He has been wearing contact lenses for 4 years and occasionally forgets to remove them at night. He has no history of serious medical illness. On examination, the patient appears distressed with pain and photophobia in the left eye. Administration of a topical anesthetic relieves the pain. Visual acuity is 20/20 in both eyes. Ocular motility and pupillary response are normal. The corneal reflex is normal and symmetric in both eyes. Which of the following is most likely to establish the diagnosis in this patient?
A 53-year-old male presents to your office for abdominal discomfort. The patient states he first noticed pain on his right flank several months ago, and it has been gradually getting worse. For the past week, he has also noticed blood in his urine. Prior to this episode, he has been healthy and does not take any medications. The patient denies fever, chills, and dysuria. He has a 40 pack-year smoking history. Vital signs are T 37 C, BP 140/90 mmHg, HR 84/min, RR 14/min, O2 98%. Physical exam is unremarkable. CBC reveals a hemoglobin of 17 and hematocrit of 51%, and urinalysis is positive for red blood cells, negative for leukocytes. Which of the following is the most likely diagnosis?
A 54-year-old man is brought by his family to the emergency department because of severe pain and weakness in his right leg. His symptoms have been gradually worsening over the past 5 weeks, but he did not seek medical care until today. He has a history of lower back pain and has no surgical history. He denies tobacco or alcohol use. His temperature is 37°C (98.6°F), the blood pressure is 140/85 mm Hg, and the pulse is 92/min. On physical examination, pinprick sensation is absent in the perineum and the right lower limb. Muscle strength is 2/5 in the right lower extremity and 4/5 in the left lower extremity. Ankle and knee reflexes are absent on the right side but present on the left. In this patient, magnetic resonance imaging (MRI) of the lumbar spine will most likely show which of the following?
A 52-year-old man is brought to the emergency department with a 2-hour history of severe, sudden-onset generalized headache. He has since developed nausea and has had one episode of vomiting. The symptoms began while he was at home watching television. Six days ago, he experienced a severe headache that resolved without treatment. He has hypertension and hyperlipidemia. The patient has smoked two packs of cigarettes daily for 30 years. His current medications include lisinopril-hydrochlorothiazide and simvastatin. His temperature is 38.1°C (100.6°F), pulse is 82/min, respirations are 16/min, and blood pressure is 162/98 mm Hg. The pupils are equal, round, and reactive to light. Fundoscopic examination shows no swelling of the optic discs. Cranial nerves II–XII are intact. He has no focal motor or sensory deficits. Finger-to-nose and heel-to-shin testing are normal. A CT scan of the head shows no abnormalities. Which of the following is the most appropriate next step in management?
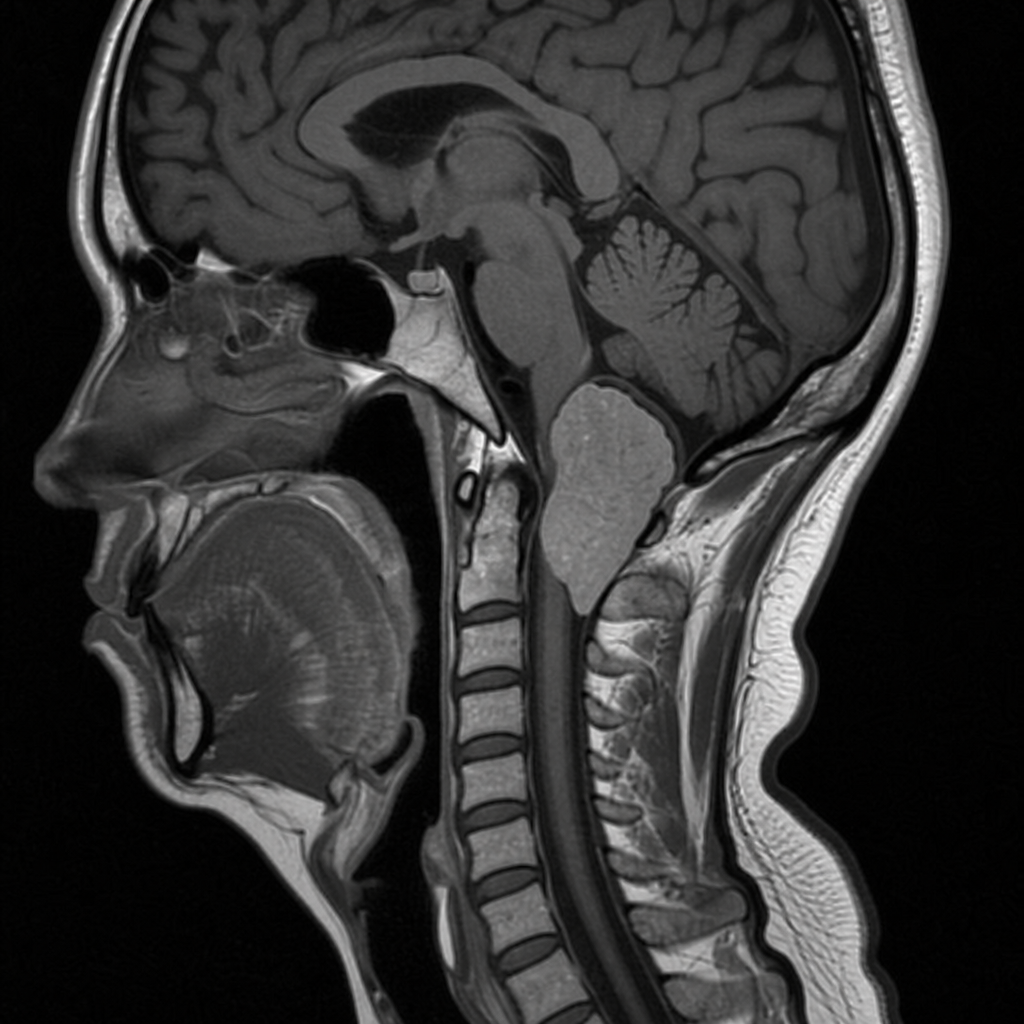
A 63-year-old woman comes to the office because of a 2-year history of upper and lower extremity weakness and neck pain that is worse with sneezing. She has had difficulty swallowing and speaking for the past 8 months. Musculoskeletal examination shows spasticity and decreased muscle strength in all extremities. There is bilateral atrophy of the trapezius and sternocleidomastoid muscles. Neurologic examination shows an ataxic gait and dysarthria. Deep tendon reflexes are 4+ bilaterally. Babinski sign is positive. Sensation is decreased below the C5 dermatome bilaterally. An MRI of the neck and base of the skull is shown. Which of the following is the most likely cause of this patient's symptoms?
A 37-year-old woman presents to the Emergency Department after 8 hours of left sided flank pain that radiates to her groin and pelvic pain while urinating. Her medical history is relevant for multiple episodes of urinary tract infections, some requiring hospitalization, and intravenous antibiotics. In the hospital, her blood pressure is 125/83 mm Hg, pulse of 88/min, a respiratory rate of 28/min, and a body temperature of 36.5°C (97.7°F). On physical examination, she has left costovertebral tenderness and lower abdominal pain. Laboratory studies include a negative pregnancy test, mild azotemia, and a urinary dipstick that is positive for blood. Which of the following initial tests would be most useful in the diagnosis of this case?
A 25-year-old woman presents with slightly yellow discoloration of her skin and eyes. She says she has had multiple episodes with similar symptoms before. She denies any recent history of nausea, fatigue, fever, or change in bowel/bladder habits. No significant past medical history. The patient is afebrile and vital signs are within normal limits. On physical examination, she is jaundiced, and her sclera is icteric. Laboratory findings are significant only for a mild unconjugated hyperbilirubinemia. The remainder of laboratory results is unremarkable. Which of the following is the most likely diagnosis in this patient?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app