
Differential diagnosis — MCQs

On this page
A 63-year-old woman comes to the emergency department because of a 1-day history of progressive blurring and darkening of her vision in the right eye. Upon waking up in the morning, she suddenly started seeing multiple dark streaks. She has migraines and type 2 diabetes mellitus diagnosed at her last health maintenance examination 20 years ago. She has smoked one pack of cigarettes daily for 40 years. Her only medication is sumatriptan. Her vitals are within normal limits. Ophthalmologic examination shows visual acuity of 20/40 in the left eye and 20/100 in the right eye. The fundus is obscured and difficult to visualize on fundoscopic examination of the right eye. The red reflex is diminished on the right. Which of the following is the most likely diagnosis?
A 32-year-old woman with a recurrent vesicular genital rash comes to the physician because of a 3-day history of a painful, pruritic rash that began on the extremities and has spread to her trunk. Her only medication is acyclovir. Her temperature is 38.1°C (100.6°F). Examination of the skin shows several reddish-purple papules and macules, some of which have a dusky center with a lighter ring around them. Which of the following is the most likely diagnosis?
A 33-year-old woman comes to the physician because of vision impairment in her right eye for the past 2 weeks. During this period, she was unable to distinguish colors with her right eye. She also reports pain with eye movement. She has no double vision. She occasionally has headaches that are relieved by ibuprofen. One year ago, she had a similar episode that affected her left eye and resolved spontaneously. She has no history of serious illness. She works at a library and enjoys reading, even in poor lighting conditions. Her vital signs are within normal limits. The pupils are equal, round, and reactive to light and accommodation. Without correction, visual acuity is 20/50 in the left eye, and 20/100 in the right eye. With spectacles, the visual acuity is 20/20 in the left eye and 20/100 in the right eye. Slit lamp examination shows no abnormalities. A CT scan of the head shows no abnormalities. Which of the following is the most likely diagnosis?
A 27-year-old young man presents to his primary care physician for weakness and tingling in his hand. The patient is an avid bodybuilder and has noticed that his grip strength has gradually worsened in both hands with symptoms worse at the end of a long workout. The patient has a past medical history of anabolic steroid use in high school. His current medications include a multivitamin, fish oil, and whey protein supplements. On physical exam, you note a muscular young man with male pattern hair loss. The patient has a loss of sensation bilaterally over the volar surface of the 4th and 5th digits and over the medial aspect of the dorsal hand. The patient has 3/5 grip strength of his left hand and 2/5 grip strength of his right hand. There is also notable weakness of finger adduction and abduction. The rest of the patient's physical exam is within normal limits. Which of the following is the most likely diagnosis?
A 75-year-old female presents to your office with her daughter. The patient states that she feels perfectly well and that she does not know why she is present. The daughter states that over the last several years, the patient has become forgetful and recently forgot her grandchild's name, along with the groceries she was supposed to buy. She was also found lost 10 miles away from her house last week. The daughter also states that the patient has had urinary incontinence over the last few months and has been seeing little children in the morning that are not present. The patient denies any recent falls. Her vitals are normal and her physical exam does not reveal any focal neurological deficits. Her mini-mental status exam is scored 22/30. What is the most accurate test for this patient?
A 7-year-old girl comes in to the emergency department with her mother for swelling of her left periorbital region. Yesterday morning she woke up with a painful, warm, soft lump on her left eyelid. Eye movement does not worsen the pain. Physical examination shows redness and swelling of the upper left eyelid, involving the hair follicles. Upon palpation, the swelling drains purulent fluid. Which of the following is the most likely diagnosis?
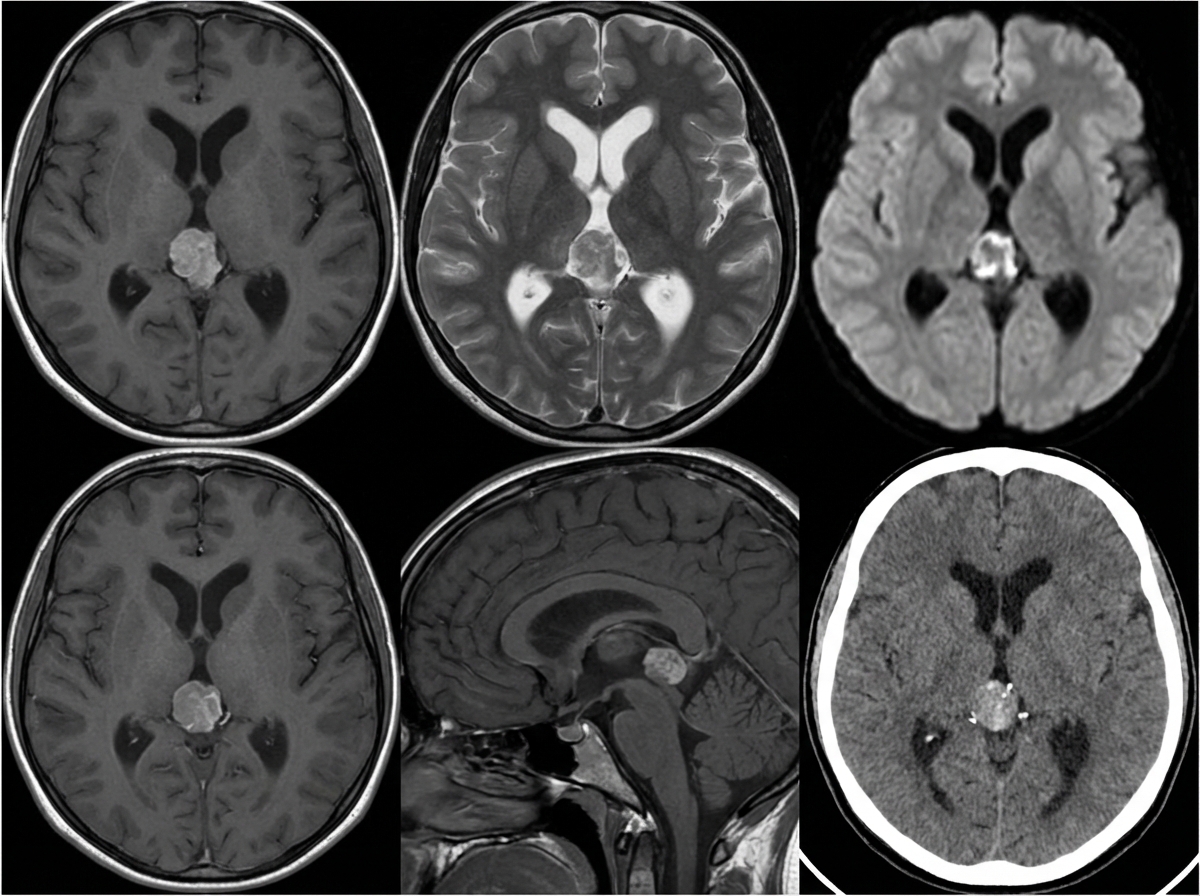
A 10-year-old girl is brought to the physician by her parents due to 2 months of a progressively worsening headache. The headaches were initially infrequent and her parents attributed them to stress from a recent move. However, over the last week the headaches have gotten significantly worse and she had one episode of vomiting this morning when she woke up. Her medical history is remarkable for a hospitalization during infancy for bacterial meningitis. On physical exam, the patient has difficulty looking up. The lower portion of her pupil is covered by the lower eyelid and there is sclera visible below the upper eyelid. A magnetic resonance imaging (MRI) of the brain is shown. Which of the following is the most likely diagnosis?
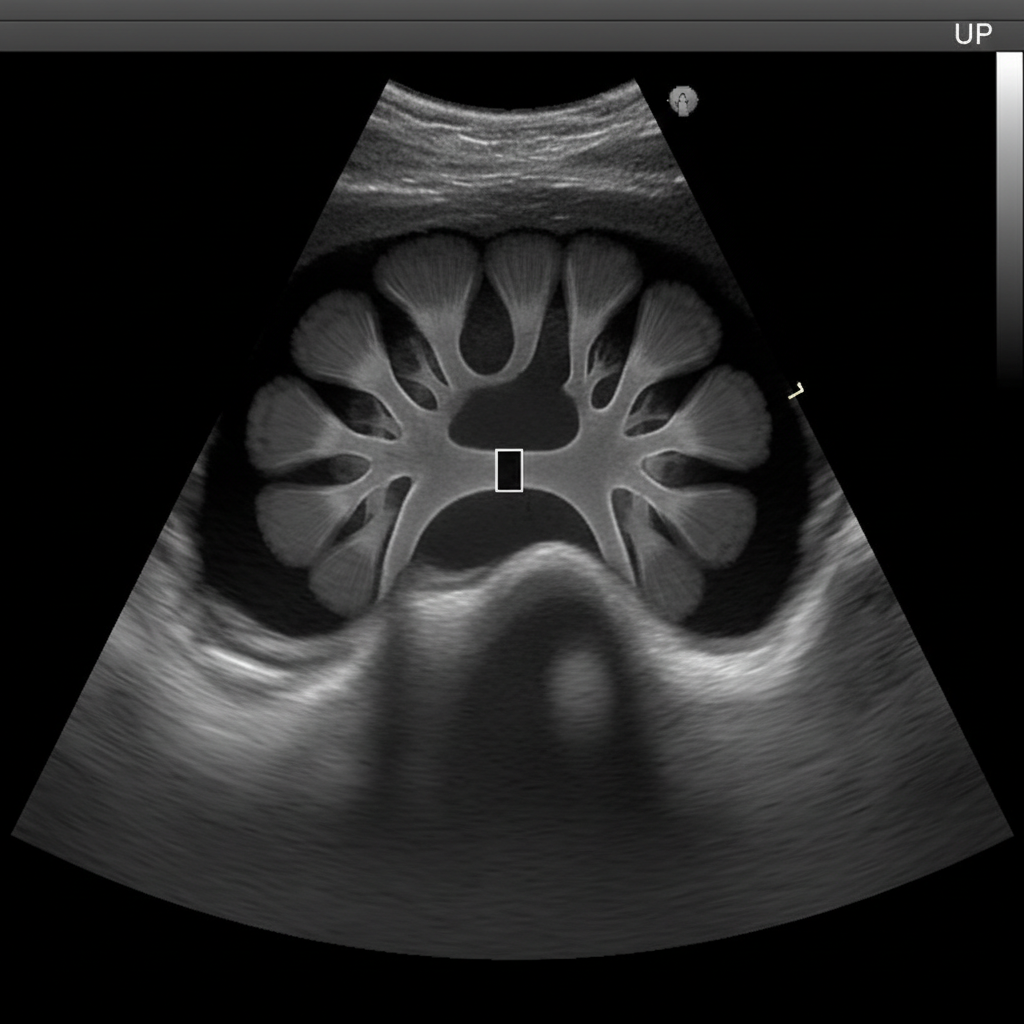
A 32-year-old female presents with acute onset abdominal pain accompanied by nausea, vomiting, and hematuria. She is currently taking glipizide for type 2 diabetes mellitus. Past medical history is also significant for lactose intolerance. She has just started training for a marathon, and she drinks large amounts of sports drinks to replenish her electrolytes and eats a high-protein diet to assist in muscle recovery. She admits to using laxatives sporadically to help her manage her weight. On physical exam, the patient appears distressed and has difficulty getting comfortable. Her temperature is 36.8°C (98.2°F), heart rate is 103/min, respiratory rate is 15/min, blood pressure is 105/85 mm Hg, and oxygen saturation is 100% on room air. Her BMI is 21 kg/m2. CBC, CMP, and urinalysis are ordered. Renal ultrasound demonstrates hydronephrosis consistent with an obstruction at the ureteropelvic junction (see image). Which of the following would most likely be seen in this patient?
A 64-year-old woman comes to the physician for a follow-up examination. She has had difficulty reading for the past 6 months. She tried using multiple over-the-counter glasses with different strengths, but they have not helped. She has hypertension and type 2 diabetes mellitus. Current medications include insulin and enalapril. Her temperature is 37.1°C (98.8°F), pulse is 80/min, and blood pressure is 126/84 mm Hg. The pupils are round and react sluggishly to light. Visual acuity in the left eye is 6/60 and in the right eye counting fingers at 6 feet. Fundoscopy shows pallor of the optic disc bilaterally. The cup-to-disk ratio is 0.7 in the left eye and 0.9 in the right eye (N = 0.3). Which of the following is the most likely diagnosis?
A 25-year-old man presents to the emergency department with the sudden onset of neck pain and a severe spinning sensation for the last 6 hours. The symptoms initially began while he was lifting weights in the gym. He feels the room is spinning continuously, and he is unable to open his eyes or maintain his balance. The dizziness and pain are associated with nausea and vomiting. Past medical history is unremarkable. His blood pressure is 124/88 mm Hg, the heart rate is 84/min, the temperature is 37.0°C (98.6°F), the respiratory rate is 12/min, and the BMI is 21.6 kg/m2. On physical examination, he is awake and oriented to person, place, and time. Higher mental functions are intact. There are several horizontal beats of involuntary oscillatory eye movements on the left lateral gaze. He has difficulty performing repetitive pronation and supination movements on the left side. Electrocardiogram reveals normal sinus rhythm. Which of the following additional clinical features would you expect to be present?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app