
Differential diagnosis — MCQs

On this page
A 52-year-old woman presents to the urgent care center with several hours of worsening abdominal discomfort that radiates to the back. The patient also complains of malaise, chills, nausea, and vomiting. Social history is notable for alcoholism. On physical exam, she is febrile to 39.5°C (103.1℉), and she is diffusely tender on abdominal palpation. Other vital signs include a blood pressure of 126/74 mm Hg, heart rate of 74/min, and respiratory rate of 14/min. Complete blood count is notable for 13,500 white blood cells (WBCs), and her complete metabolic panel shows bilirubin of 2.1 and amylase of 3210. Given the following options, what is the most likely diagnosis?
A 66-year-old man is transferred from another hospital after 3 days of progressively severe headache, vomiting, low-grade fever, and confusion. According to his partner, the patient has been dealing with some memory loss and complaining about headaches for the past 2 weeks. He has a history of interstitial pulmonary disease that required lung transplantation 2 years ago. Upon admission, he is found with a blood pressure of 160/100 mm Hg, a pulse of 58/min, a respiratory rate of 15/min, and a body temperature of 36°C (97°F). During the examination, he is found with oral thrush and symmetric and reactive pupils; there are no focal neurological signs or papilledema. A lumbar puncture is performed. Which of the following features would be expected to be found in this case?
A 19-year-old man with a past medical history significant only for moderate facial acne and mild asthma presents to his primary care physician with a new rash. He notes it has developed primarily over the backs of his elbows and is itchy. He also reports a 6-month history of foul-smelling diarrhea. He has no significant social or family history. The patient's blood pressure is 109/82 mm Hg, pulse is 66/min, respiratory rate is 16/min, and temperature is 36.7°C (98.0°F). Physical examination reveals crusting vesicular clusters on his elbows with a base of erythema and edema. What is the most likely underlying condition?
A 37‐year‐old woman presents with a severe, deep, sharp pain in her right hand and forearm. A week before she presented her pain symptoms, she fell on her right forearm and developed mild bruising. She has type-1 diabetes mellitus and is on an insulin treatment. The physical examination reveals that her right hand and forearm were warmer, more swollen, and had a more reddish appearance than the left side. She feels an intense pain upon light touching of her right hand and forearm. Her radial and brachial pulses are palpable. The neurological examination is otherwise normal. The laboratory test results are as follows: Hemoglobin 15.2 g/dL White blood cell count 6,700 cells/cm3 Platelets 300,000 cells/cm3 Alanine aminotransferase 32 units/L Aspartate aminotransferase 38 units/L C-reactive protein 0.4 mg/L Erythrocyte sedimentation rate 7 mm/1st hour The X-ray of the right hand and forearm do not show a fracture. The nerve conduction studies are also within normal limits. What is the most likely diagnosis?
A 25-year-old male presents to his primary doctor with difficulty sleeping. On exam, he is noted to have impaired upgaze bilaterally, although the rest of his ocular movements are intact. On pupillary exam, both pupils accommodate, but do not react to light. What is the most likely cause of his symptoms?
A 72-year-old man is brought into clinic by his daughter for increasing confusion. The daughter states that over the past 2 weeks, she has noticed that the patient “seems to stare off into space.” She reports he has multiple episodes a day during which he will walk into a room and forget why. She is also worried about his balance. She endorses that he has had several falls, the worst being 3 weeks ago when he tripped on the sidewalk getting the mail. The patient denies loss of consciousness, pre-syncope, chest pain, palpitations, urinary incontinence, or bowel incontinence. He complains of headache but denies dizziness. He reports nausea and a few episodes of non-bloody emesis but denies abdominal pain, constipation, or diarrhea. The patient’s medical history is significant for atrial fibrillation, diabetes, hypertension, hyperlipidemia, and osteoarthritis. He takes aspirin, warfarin, insulin, lisinopril, simvastatin, and ibuprofen. He drinks a half glass of whisky after dinner every night and smokes a cigar on the weekends. On physical examination, he is oriented to name and place but not to date. He is unable to spell "world" backward. When asked to remember 3 words, he recalls only 2. There are no motor or sensory deficits. Which of the following is the most likely diagnosis?
An otherwise healthy 62-year-old woman comes to the physician because of a 3-year history of hearing loss. To test her hearing, the physician performs two tests. First, a vibrating tuning fork is held against the mastoid bone of the patient and then near her ear, to which the patient responds she hears the sound better on both sides when the tuning fork is held near her ear. Next, the physician holds the tuning fork against the bridge of her forehead, to which the patient responds she hears the sound better on the right side than the left. The patient's examination findings are most consistent with which of the following conditions?
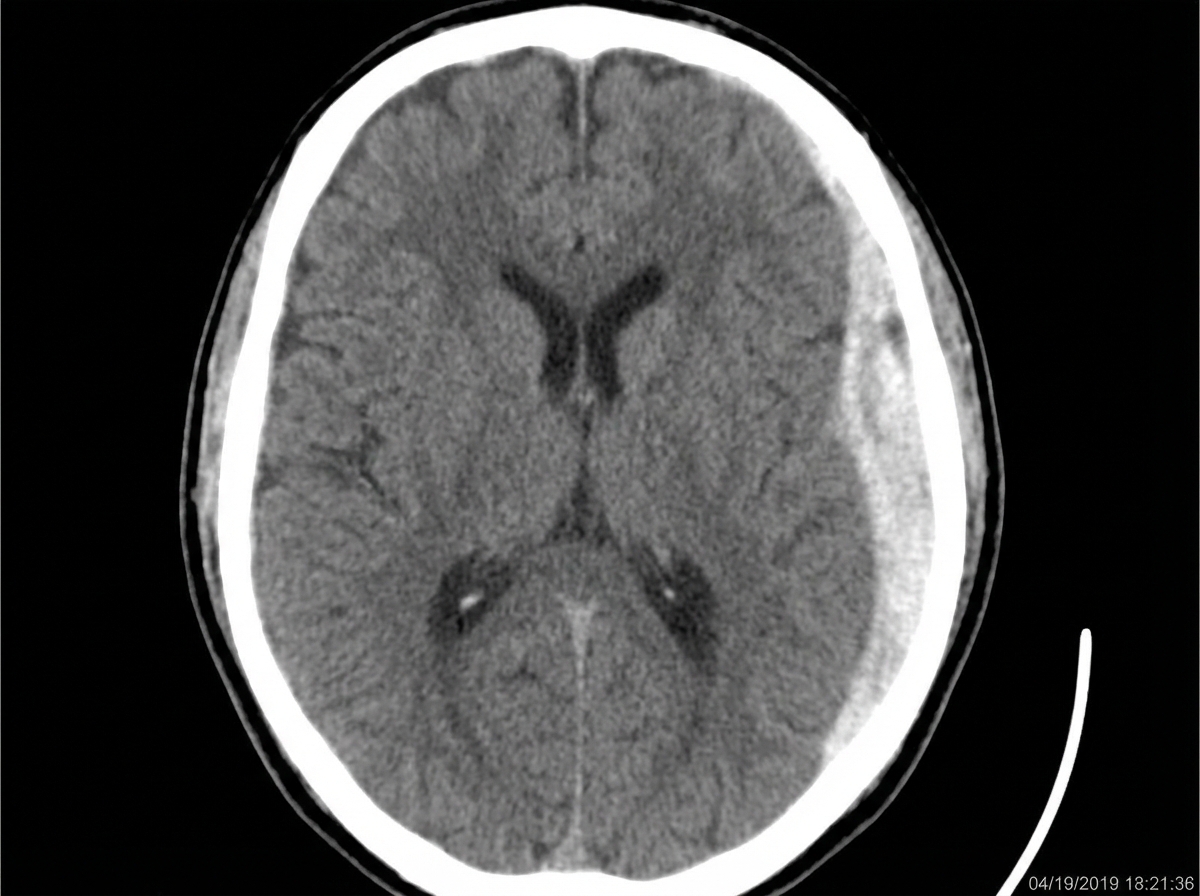
A 68-year-old community-dwelling woman is transported to the emergency department with decreased consciousness, headache, and nausea. The symptoms began after the patient had a syncopal episode and fell at her home. She has a history of arterial hypertension and atrial fibrillation. Her current medications include hydrochlorothiazide, lisinopril, metoprolol, and warfarin. On admission, her blood pressure is 140/90 mm Hg, heart rate is 83/min and irregular, respiratory rate is 12/min, and temperature is 36.8°C (98.4°F). She is conscious and verbally responsive, albeit confused. She is able to follow motor commands. Her pupils are round, equal, and poorly reactive to light. She is unable to abduct both eyes on an eye movement examination. She has decreased strength and increased tone (Ashworth 1/4) and reflexes (3+) in her right upper and lower extremities. Her lungs are clear to auscultation. The cardiac examination shows the presence of S3 and a pulse deficit. A head CT scan is shown in the picture. Which of the following led to the patient’s condition?
A 43-year-old man presents with acute-onset left flank pain for the past 6 hours. He describes the pain as severe, intermittent, colicky, and “coming in waves”, and he points to the area of the left costovertebral angle (CVA). He says he recently has been restricting oral liquid intake to only 2 glasses of water per day based on the advice of his healer. He also reports nausea and vomiting. The patient has a history of hypertension, gout, and type 2 diabetes mellitus. He is afebrile, and his vital signs are within normal limits. On physical examination, he is writhing in pain and moaning. There is exquisite left CVA tenderness. A urinalysis shows gross hematuria. Which of the following is the next best step in the management of this patient?
A 55-year-old man presents to the emergency department for severe pain in his knee. The patient states that the pain began yesterday and has steadily worsened. The patient has a history of osteoarthritis of the knee, which was previously responsive to ibuprofen. He reports taking 3 doses of hydrochlorothiazide today after not taking his medication for 3 days. He recently attended a barbecue, which entailed eating beef and drinking alcohol. The patient was also recently treated for cellulitis. The patient has a past medical history of obesity, diabetes, and osteoarthritis. His temperature is 101°F (38.3°C), blood pressure is 157/98 mmHg, pulse is 95/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam is notable for a warm and erythematous left knee. There is tenderness to palpation of the left knee with limited range of motion due to pain. Which of the following is the best next step in management?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app