
Differential diagnosis — MCQs

On this page
A 24-year-old female presents to her primary care physician with right knee pain for the last week. She states that she first noticed it after a long flight on her way back to the United States from Russia, where she had run a marathon along a mountain trail. The patient describes the pain as dull, aching, and localized to the front of her kneecap, and it worsens with sitting but improves with standing. Aspirin has not provided significant relief. The patient has a history of a torn anterior cruciate ligament (ACL) on the right side from a soccer injury three years ago. In addition, she was treated for gonorrhea last month after having intercourse with a new partner. At this visit, the patient’s temperature is 98.5°F (36.9°C), blood pressure is 112/63 mmHg, pulse is 75/min, and respirations are 14/min. Which of the following is most likely to establish the diagnosis?
A 48-year-old man with a history of nephrolithiasis presents with acute-onset left flank pain. He says that the pain started suddenly 4 hours ago and has progressively worsened. He describes the pain as severe, sharp, and localized to the left flank. The patient denies any fever, chills, nausea, vomiting, or dysuria. His past medical history is significant for nephrolithiasis diagnosed 4 years ago status post shockwave lithotripsy. The patient says, "I’m allergic to many pain medications, but there is one that I get all the time when I have this pain. I think it starts with D". He is afebrile and his vital signs are stable. On physical examination, he is writhing in pain and moaning. Exquisite left costovertebral angle tenderness is noted. Laboratory findings, including a urinalysis, are unremarkable. IV fluid resuscitation is administered. Which of the following is the best next step in the management of this patient?
A 47-year-old male with a medical history significant for hypertension, recurrent urinary tract infections, mitral valve prolapse, and diverticulosis experiences a sudden, severe headache while watching television on his couch. He calls 911 and reports to paramedics that he feels as if "someone shot me in the back of my head." He is rushed to the emergency room. On exam, he shows no focal neurological deficits but has significant nuchal rigidity and photophobia. Of the options below, what is the most likely etiology of this man's headache?
A 23-year-old man presents to the emergency department with a severe headache. The patient states he gets sudden, severe pain over his face whenever anything touches it, including shaving or putting lotion on his skin. He describes the pain as electric and states it is only exacerbated by touch. He is currently pain free. His temperature is 98.1°F (36.7°C), blood pressure is 127/81 mmHg, pulse is 87/min, respirations are 15/min, and oxygen saturation is 98% on room air. Neurological exam is within normal limits, except severe pain is elicited with light palpation of the patient’s face. The patient is requesting morphine for his pain. Which of the following is the most likely diagnosis?
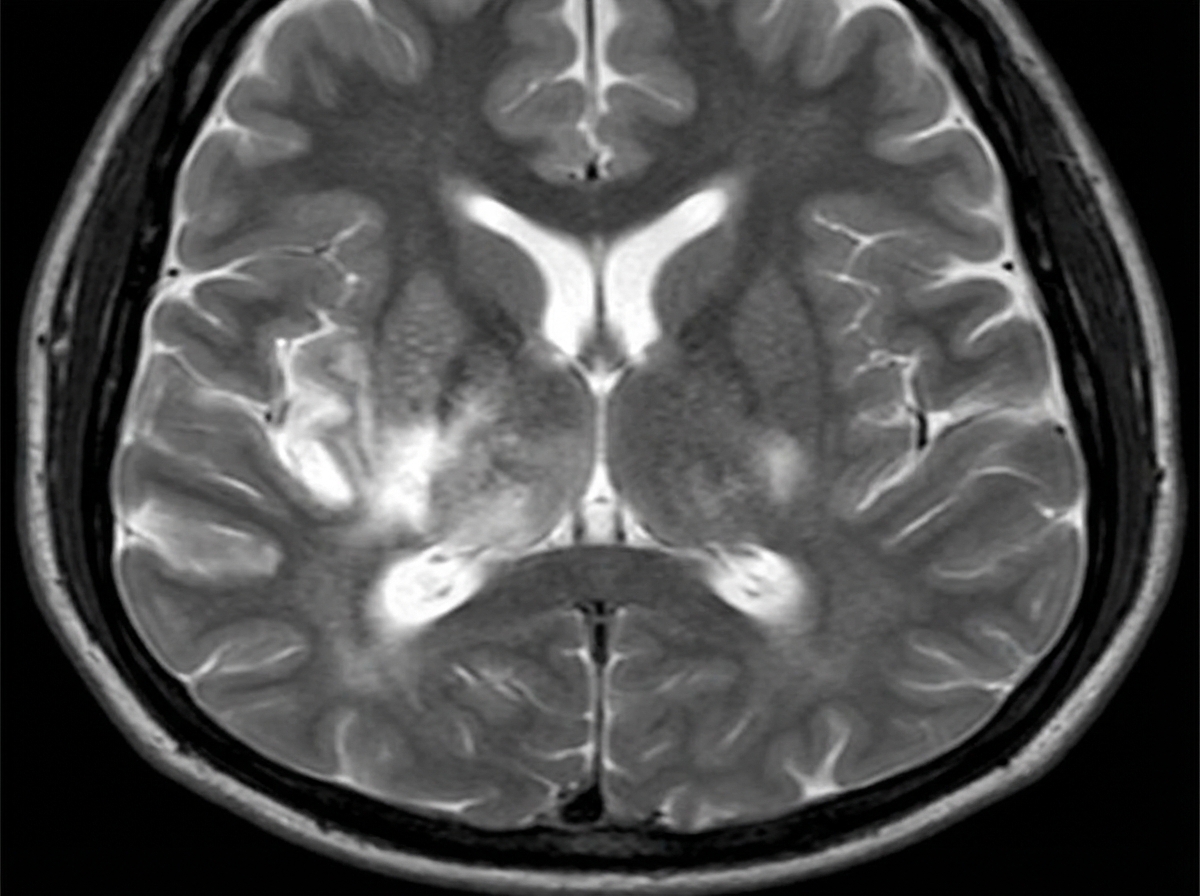
A 24-year-old man is brought to the emergency department after he is found sluggish, drowsy, feverish, and complaining about a headache. His past medical history is unremarkable. His vital signs include: blood pressure 120/60 mm Hg, heart rate 70/min, respiratory rate 17/min, and body temperature 39.0°C (102.2°F). On physical examination, the patient is dysphasic and incapable of following commands. Gait ataxia is present. No meningeal signs or photophobia are present. A noncontrast CT of the head is unremarkable. A T2 MRI is performed and is shown in the image. A lumbar puncture (LP) is subsequently performed. Which of the following CSF findings would you most likely expect to find in this patient?
A 59-year-old woman comes to the emergency department 25 minutes after the onset of severe left periorbital pain and blurred vision in the same eye. The pain began soon after she entered a theater to watch a movie. She has a headache and vomited twice on the way to the hospital. Two weeks ago, she had acute sinusitis that resolved spontaneously. She has atrial fibrillation and hypertension. Current medications include metoprolol and warfarin. Her temperature is 37.1°C (98.8°F), pulse is 101/min, and blood pressure is 140/80 mm Hg. Visual acuity is counting fingers at 3 feet in the left eye and 20/20 in the right eye. The left eye shows conjunctival injection and edematous cornea. The left pupil is mid-dilated and irregular; it is not reactive to light. Extraocular movements are normal. Fundoscopic examination is inconclusive because of severe corneal edema. Which of the following is the most likely diagnosis?
A 12-year-old boy is brought to the office by his mother with complaints of clear nasal discharge and cough for the past 2 weeks. The mother says that her son has pain during swallowing. Also, the boy often complains of headaches with a mild fever. Although his mother gave him some over-the-counter medication, there was only a slight improvement. Five days ago, his nasal discharge became purulent with an increase in the frequency of his cough. He has no relevant medical history. His vitals include: heart rate 95 bpm, respiratory rate 17/min, and temperature 37.9°C (100.2°F). On physical exploration, he has a hyperemic pharynx with purulent discharge on the posterior wall, halitosis, and nostrils with copious amounts of pus. Which of the following is the most likely cause?
A 31-year-old obese Caucasian female presents to the Emergency Department late in the evening for left lower quadrant pain that has progressively worsened over the last several hours. She describes the pain as sharp and shooting, coming and going. Her last bowel movement was this morning. She has also had dysuria and urgency. Her surgical history is notable for gastric bypass surgery 2 years prior and an appendectomy at age 9. She is sexually active with her boyfriend and uses condoms. Her temperature is 99.5 deg F (37.5 deg C), blood pressure is 151/83 mmHg, pulse is 86/min, respirations are 14/minute, BMI 32. On physical exam, she has left lower quadrant tenderness to palpation with pain radiating to the left groin and left flank tenderness on palpation. Her urinalysis shows 324 red blood cells/high power field. Her pregnancy test is negative. What is the next best step in management?
A 16-year-old girl is brought to the physician because of yellowish discoloration of her eyes and generalized fatigue since she returned from a 2-week class trip to Guatemala 2 days ago. During her time there, she had watery diarrhea, nausea, and lack of appetite for 3 days that resolved without treatment. She also took primaquine for malaria prophylaxis. Three weeks ago, she had a urinary tract infection that was treated with nitrofurantoin. Her immunizations are up-to-date. Her temperature is 37.1°C (98.8°F), pulse is 82/min and blood pressure is 110/74 mm Hg. Examination shows scleral icterus. There is no lymphadenopathy. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 12.1 g/dL Leukocyte count 6400/mm3 Platelet count 234,000/mm3 Reticulocyte count 1.1% Prothrombin time 12 sec (INR=1) Serum Bilirubin Total 2.8 mg/dL Direct 0.2 mg/dL Alkaline phosphatase 43 U/L AST 16 U/L ALT 17 U/L γ-Glutamyltransferase 38 U/L (N = 5–50) Anti-HAV IgG positive Anti-HBs positive A peripheral blood smear shows no abnormalities. Which of the following is the most likely diagnosis?
A 16-year-old boy is brought to the physician by his mother because of a 4-day history of painful lesions in his mouth. During the past year, he has twice had similar lesions that resolved without treatment after approximately 10 days. He has never had any genital or anal lesions. His mother reports that he has been very stressed over the past month because he is approaching his senior year at high school. He is otherwise healthy and takes no medications. He appears thin. His temperature is 37.6°C (99.7°F). A photograph of his oral cavity is shown. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?

Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app