
Differential diagnosis — MCQs

On this page
A 16-year-old boy is brought to the physician for a follow-up appointment. He has a seizure disorder treated with valproic acid. He has always had difficulties with his schoolwork. He was able to walk independently at the age of 2 years and was able to use a fork and spoon at the age of 3 years. Ophthalmic examination shows hyperpigmented iris nodules bilaterally. A photograph of his skin examination findings is shown. This patient is at increased risk for which of the following conditions?

A 30-year-old woman comes to the physician because of a swelling on her neck for 5 months. It has gradually enlarged in size and is mildly painful. She has also had intermittent episodes of throbbing headache, sweating, and palpitations over the past 3 months. Menses occur at regular 28-day intervals and last for 4–5 days. She does not smoke, occasionally consumes alcohol on weekends. She appears thin and pale. Her temperature is 38.7°C (101.7°F), pulse is 112/min, and blood pressure is 140/90 mm Hg. Examination shows a firm, 3-cm swelling on the neck that moves with swallowing; there is no lymphadenopathy. Cardiopulmonary examination shows no abnormalities. Laboratory studies show: Hemoglobin 13 g/dL Leukocyte count 9500/mm3 Platelet count 230,000/mm3 Serum Na+ 136 mEq/L K+ 3.5 mEq/L Cl- 104 mEq/L TSH 2.3 μU/mL Calcitonin 300 ng/dL (Normal < 5 ng/dL) An electrocardiogram shows sinus tachycardia. Which of the following laboratory abnormalities is most likely to be seen?
A 50-year-old man comes to the physician for a routine checkup. He has had a progressively increasing swelling on the nape of his neck for 2 months. He does not have a fever or any discharge from the swelling. He underwent a colectomy for colon cancer at the age of 43 years. He has type 2 diabetes mellitus, hypertension, and osteoarthritis of the left knee. Current medications include insulin glargine, metformin, enalapril, and naproxen. He has worked as a traffic warden for the past 6 years and frequently plays golf. He appears healthy. His temperature is 37.3°C (99.1°F), pulse is 88/min, and blood pressure is 130/86 mm Hg. Examination of the neck shows a 2.5-cm (1-in) firm, mobile, and painless nodule. The skin over the nodule cannot be pinched. The lungs are clear to auscultation. The remainder of the examination shows no abnormalities. A photograph of the lesion is shown. Which of the following is the most likely diagnosis?

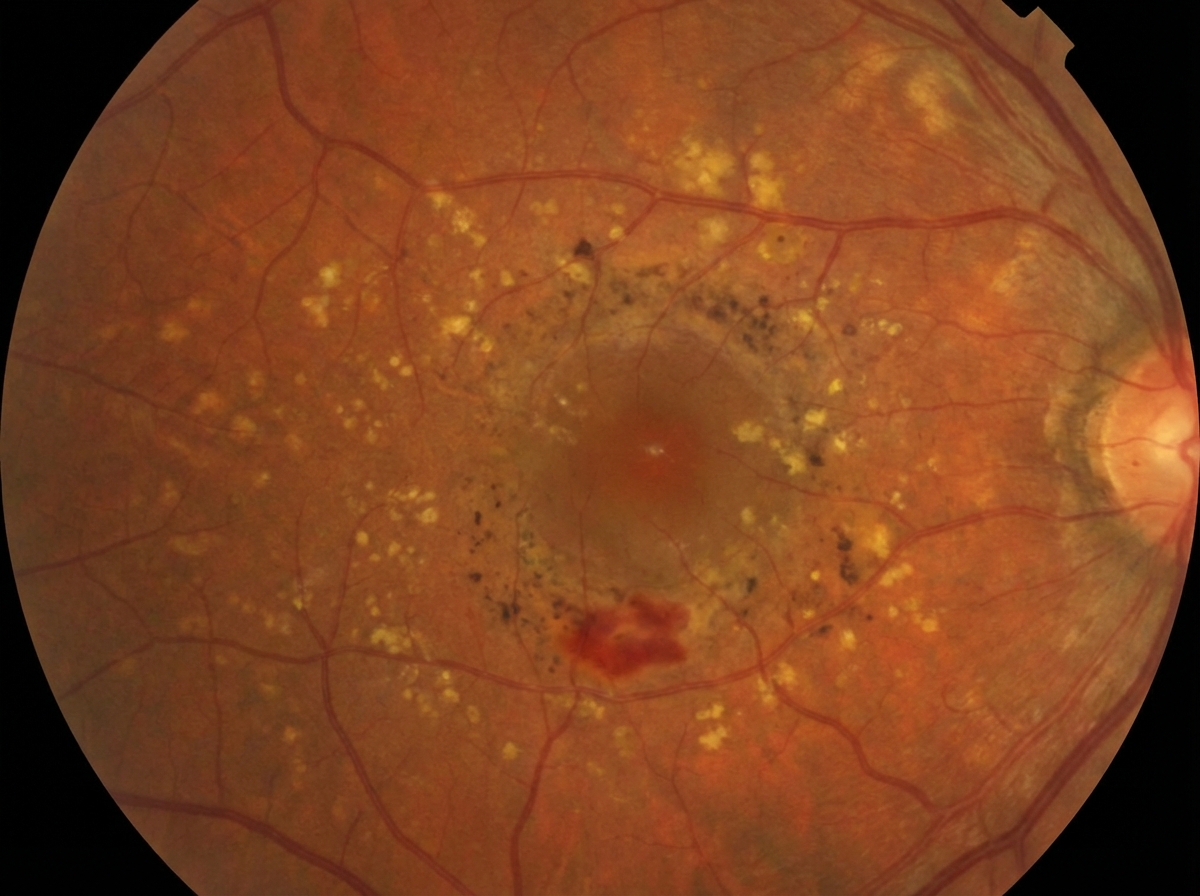
A 62-year-old woman comes to the physician because of increasing blurring of vision in both eyes. She says that the blurring has made it difficult to read, although she has noticed that she can read a little better if she holds the book below or above eye level. She also requires a bright light to look at objects. She reports that her symptoms began 8 years ago and have gradually gotten worse over time. She has hypertension and type 2 diabetes mellitus. Current medications include glyburide and lisinopril. When looking at an Amsler grid, she says that the lines in the center appear wavy and bent. An image of her retina, as viewed through fundoscopy is shown. Which of the following is the most likely diagnosis?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app