
Differential diagnosis — MCQs

On this page
A 65-year-old woman comes to the clinic for an annual well-check. Her past medical history includes diabetes and hypertension, which are well-controlled with metformin and losartan, respectively. The patient reports a healthy diet consisting of mainly vegetables and lean meat. She denies smoking or alcohol use. She enjoys taking walks with her husband and sunbathing. Physical examination is unremarkable except for a rough, scaly, sandpaper-like plaque on her left dorsal hand with no tenderness or pain. What is the most likely diagnosis?
A 28-year-old female presents to her primary care physician because of pain on her right foot. She says that the pain began 2 weeks ago and gets worse with weight bearing. She has been training for a marathon, and this pain has limited her training. On exam, there are no signs of inflammation or deformities on her foot. Compression of the forefoot with concomitant pressure on the interdigital space reproduces the pain on the plantar surface between the third and fourth toes and produces an audible click. What is the cause of this patient's condition?
A 46-year-old male presents with his wife to his primary care provider for depression and strange movements. His wife reports that her husband has not been himself for the last two months. Whereas he was previously outgoing and “the life of the party,” the patient is now irritable and withdrawn. He is a partner at an accounting firm, but his colleagues are threatening his job if he continues to perform poorly at work. The patient cannot explain the recent changes to his mood and tearfully admits he fears there is something seriously wrong with him. His wife says that she thinks he is getting worse. The patient’s past medical history is significant for hypertension, for which he takes lisinopril. His family history is unknown as he was adopted. The patient met his mother once, and never knew his father but was told he died in his 50's. He drinks a few glasses of wine per week and has never smoked. On physical exam, the patient has a flat affect with facial grimace and sudden jerky movements of his upper extremities. Which of the following is most likely to be seen on further workup?
A 27-year-old man presents to the emergency department with dizziness. He states he has experienced a sustained sensation of the room spinning that is low grade and constant since this morning. The patient occasionally feels nauseous and has been taking diphenydramine to sleep which helps with his symptoms. The patient is generally healthy, has no other medical conditions, and only endorses eating more garlic recently to get over a cold he had a few days ago. His temperature is 98.7°F (37.1°C), blood pressure is 122/81 mmHg, pulse is 82/min, respirations are 15/min, and oxygen saturation is 99% on room air. Physical exam is notable for a healthy man. The patient is sat upright, his head is turned slightly to the right, and he is laid back flat rapidly. This does not provoke any symptoms even when repeated on the left side. A nystagmus is notable on cranial nerve exam as well as bilateral decreased hearing. The patient’s tandem gait is unstable; however, his baseline gait appears unremarkable despite the patient stating he has a sustained sensation of imbalance. Which of the following is the most likely diagnosis?
A 44-year-old woman comes to her primary care physician with complaints of irritation and a gritty sensation in her eyes for the past few months. She denies any discharge from her eyes. She has no significant past medical or surgical history. She takes multivitamins occasionally but denies use of any other medication. On further questioning, she expresses her concerns about frequent dental caries for the past 2 years. On examination, her temperature is 37.1°C (98.8°F), blood pressure is 110/80 mm Hg, pulse rate is 74/min, and respiratory rate is 16/min. Which of the following is the most likely cause of her symptoms?
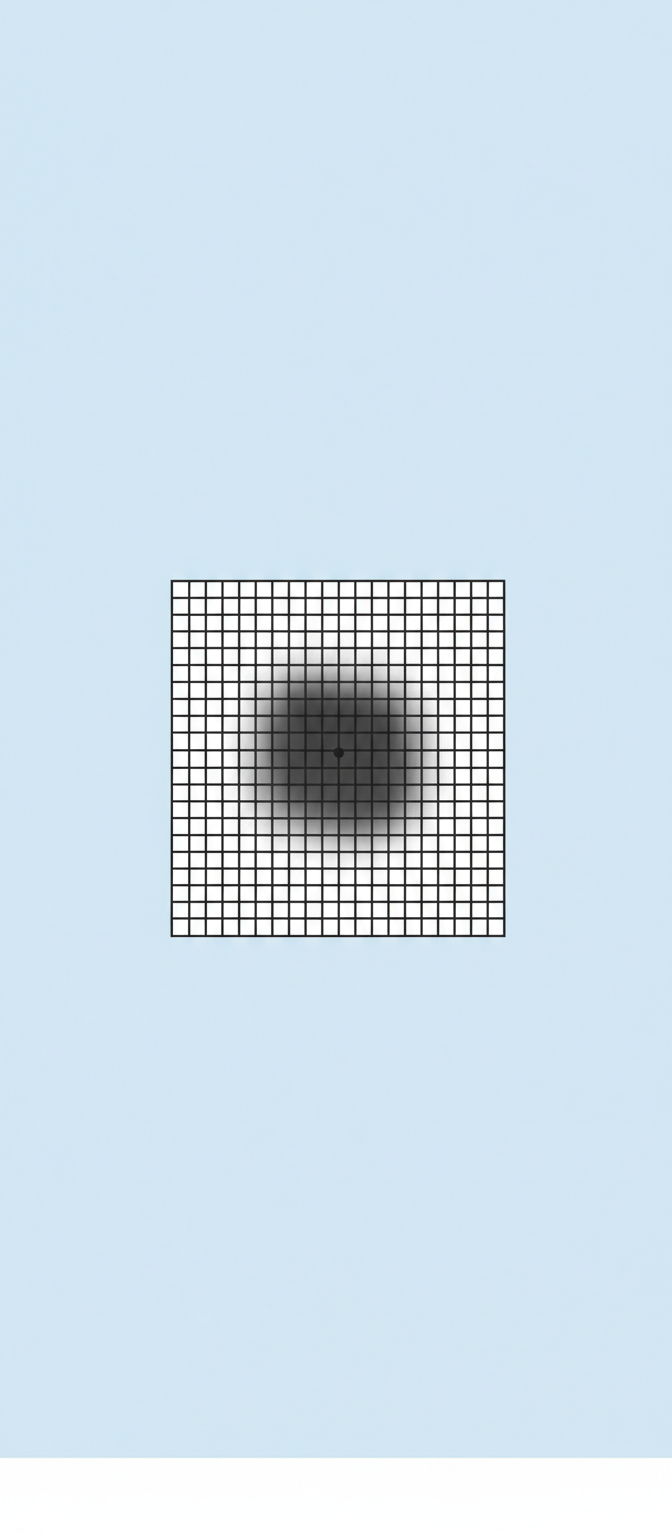
A 75-year-old man presents to the physician with progressive difficulty reading over the past year. Currently, he avoids driving as he has trouble reading road signs. He has no history of a serious illness and takes no medications. The fundoscopic examination shows localized retinal elevation and drusen. A description of the patient’s visual on the Amsler grid is shown. Fluorescein angiography shows early hyperfluorescence. Which of the following is the most likely diagnosis in this patient?
A 47-year-old man presents to the clinic for an evaluation of intense itching of his right thigh region for the past few days. He states some ‘red bumps’ just began to form. The patient mentions that he was recently at a business conference in Miami. He has a past medical history of hypertension, diabetes type 2, and hyperlipidemia. He takes enalapril, metformin, and atorvastatin. He does not smoke or drink. His vitals are within normal limits today. On physical examination, a linear line with 3 red papules is present along the medial aspect of his right thigh. Additionally, there are small rows of bumps on his left leg and right forearm. Excoriations are also apparent in the same region. Which of the following is the most likely diagnosis?
A 25-year-old woman with a history of polycystic ovarian syndrome, depression, and chronic bilateral ear infections presents to the otolaryngologist's clinic 12 weeks after right ear tympanoplasty. Her audiology report one week prior showed that her hearing improved as expected by 20 decibels. However, she reports that she has occasional shooting pain with eating and when she wears earrings. She states that she has a stressful job as a cashier at the local department store and often sleeps poorly. She denies any neck pain or tenderness when she washes her face. On physical exam, no tenderness is elicited with preauricular or mandibular palpation bilaterally. No jaw clicking is heard. Right postauricular tapping causes tenderness in her right tonsillar area. Her molar teeth appear even and symmetric bilaterally. Her uvula is midline and her gag reflex is intact. What is the most likely diagnosis?
A 69-year-old man presents to his primary care physician for pain when he walks. He states that the pain is the worst in his left great toe but is also present in his hips and knees. He says that his symptoms are worse with activity and tend to improve with rest. His symptoms have progressively worsened over the past several years. He has a past medical history of obesity, type II diabetes mellitus, smoking, and hypertension. He drinks roughly ten beers per day. His current medications include metformin, insulin, lisinopril, and hydrochlorothiazide. The patient has a recent travel history to Bangkok where he admits to having unprotected sex. On physical exam, examination of the lower extremity results in pain. There is crepitus of the patient's hip when his thigh is flexed and extended. Which of the following is the most likely diagnosis?
A 25-year-old male patient presents to your clinic in significant distress. He states he has excruciating, stabbing pain around the left side of his head, and his left eye will not stop tearing. These types of headaches have been occurring for the past week every morning when he awakens and last around 60 minutes. He denies any aura, nausea, or vomiting. He denies any other past medical history. What is this patient's diagnosis?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app