
Differential diagnosis — MCQs

On this page
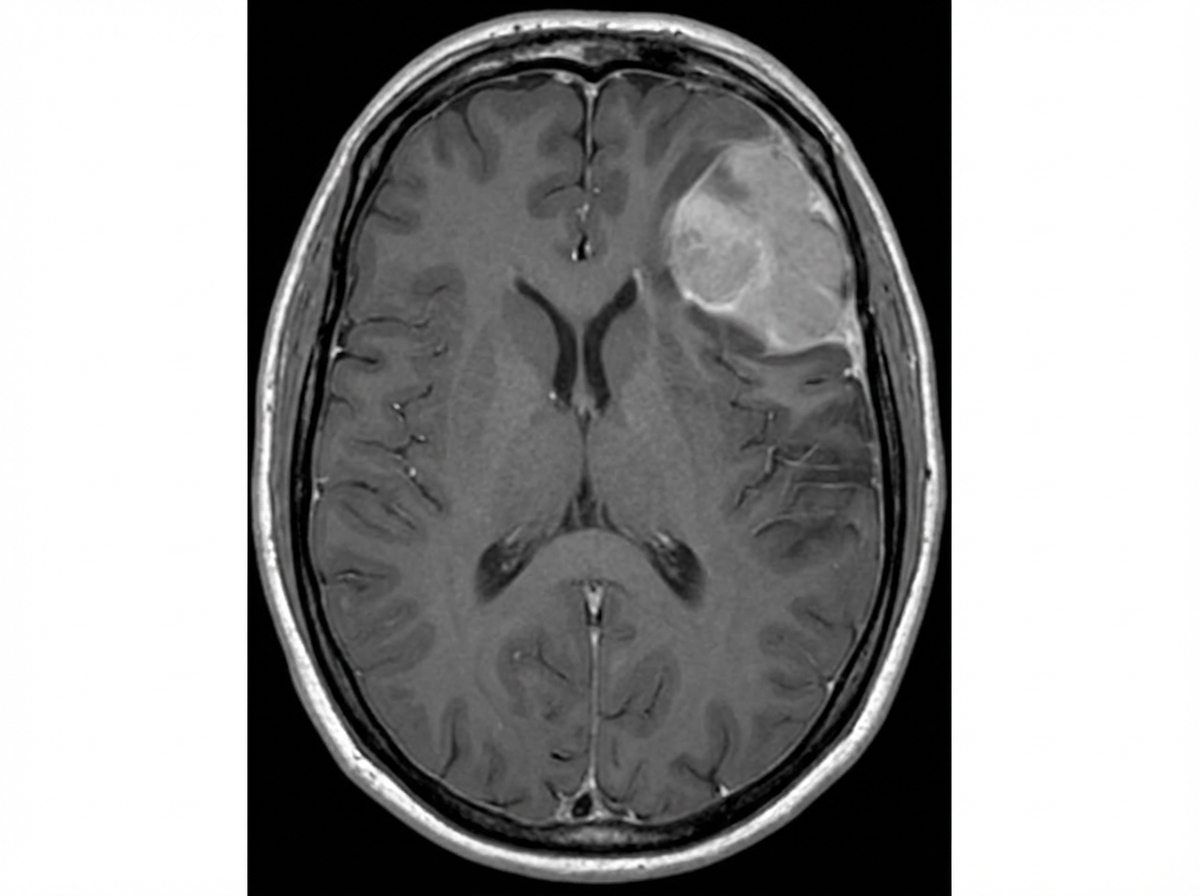
A 59-year-old man is brought to the emergency department 30 minutes after having a seizure. His wife reports that the patient has been having recurrent headaches and has become increasingly irritable over the past 3 months. Physical examination shows a spastic paresis of the right lower extremity. The Babinski sign is present on the right side. An MRI of the brain is shown. Which of the following is the most likely diagnosis?
A 75-year-old man presents to the physician because of bloody urine, which has occurred several times over the past month. He has no dysuria, flank pain, nausea, or vomiting. He has no history of serious illness and takes no medications. He is a 40-pack-year smoker. The vital signs are within normal limits. Physical exam shows no abnormalities except generalized lung wheezing. The laboratory test results are as follows: Urine Blood 3+ RBC > 100/hpf WBC 1–2/hpf RBC casts Negative Bacteria Not seen Which of the following is the most appropriate diagnostic study at this time?
A 32-year-old woman comes to the emergency department because of a 12-hour history of a severe headache. She does not smoke or use illicit drugs. Her blood pressure at admission is 180/125 mm Hg. Physical examination shows a bruit in the epigastric region. Fundoscopy shows bilateral optic disc swelling. Which of the following investigations is most likely to confirm the diagnosis?
A 57-year-old woman comes to the physician because of a 6-month history of tinnitus and progressive hearing loss in the left ear. She has type 2 diabetes mellitus and Raynaud syndrome. Her current medications include metformin, nifedipine, and a multivitamin. She appears well. Vital signs are within normal limits. Physical examination shows no abnormalities. A vibrating tuning fork is placed on the left mastoid process. Immediately after the patient does not hear a tone, the tuning fork is held over the left ear and she reports hearing the tuning fork again. The same test is repeated on the right side and shows the same pattern. The vibration tuning fork is then placed on the middle of the forehead and the patient hears the sound louder in the right ear. Which of the following is the most likely diagnosis?
A 31-year-old man comes to the physician because of pain, tingling, and numbness in his right hand that started 3 months ago. It is worse at night and frequently wakes him up. The symptoms can be relieved by shaking his hands but soon recur. He reports weakness of his right hand, especially when grasping objects. He has type 2 diabetes mellitus. His current medications are metformin and sitagliptin. Four months ago he went on a camping trip. He has been working as a hardscaper for 8 years. His temperature is 37.5°C (99.5°F), pulse is 86/min, and blood pressure is 110/70 mm Hg. Examination shows reproduction of his symptoms when his right hand is held above his head for 2 minutes. Laboratory studies show: Hemoglobin 13.2 g/dL Leukocyte count 7,600/mm3 Hemoglobin A1C 6.3% Erythrocyte sedimentation rate 13 mm/h Which of the following is most likely to confirm the diagnosis?
A 62-year-old woman is brought to the emergency department because of sudden loss of vision in her right eye that occurred 50 minutes ago. She does not have eye pain. She had several episodes of loss of vision in the past, but her vision improved following treatment with glucocorticoids. She has coronary artery disease, hypertension, type 2 diabetes mellitus, and multiple sclerosis. She underwent a left carotid endarterectomy 3 years ago. She had a myocardial infarction 5 years ago. Current medications include aspirin, metoprolol, lisinopril, atorvastatin, metformin, glipizide, and weekly intramuscular beta-interferon injections. Her temperature is 36.8°C (98.2°F), pulse is 80/min, and blood pressure is 155/88 mm Hg. Examination shows 20/50 vision in the left eye and no perception of light in the right eye. The direct pupillary reflex is brisk in the left eye and absent in the right eye. The indirect pupillary reflex is brisk in the right eye but absent in the left eye. Intraocular pressure is 18 mm Hg in the right eye and 16 mm Hg in the left eye. A white, 1-mm ring is seen around the circumference of the cornea in both eyes. Fundoscopic examination of the right eye shows a pale, white retina with a bright red area within the macula. The optic disc appears normal. Fundoscopic examination of the left eye shows a few soft and hard exudates in the superior and nasal retinal quadrants. The optic disc and macula appear normal. Which of the following is the most likely diagnosis?
A 13-year-old boy is brought to the physician because of a 1-month history of progressive difficulty breathing through his nose and a 2-week history of recurrent severe nosebleeds. When he holds the right nostril shut, he is unable to breathe nasally and his sense of smell is reduced. He has a 6-year history of asthma, which is well controlled with inhaled albuterol. Vital signs are within normal limits. Nasal inspection shows a pink, lobulated mass filling the left nasal cavity. The septum is deviated to the right side. The mass bleeds on touch. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in diagnosis?
A 50-year-old man comes to the emergency department for evaluation of right-sided facial weakness that he noticed after waking up. One month ago, he also experienced right-sided neck pain and headache that began after returning from a hunting trip to New Hampshire the week before. He took ibuprofen to relieve symptoms, which subsided a week later. He has a 5-year history of hypertension controlled with drug therapy. He has smoked one pack of cigarettes daily for 35 years and he drinks two beers daily. His vital signs are within the normal range. Physical examination shows right-sided drooping of the upper and lower half of the face. The patient has difficulties smiling and he is unable to close his right eye. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in diagnosis?
A 50-year-old woman comes to the physician because of blisters on her forearm that appeared 3 days ago. She also reports pain in her left cheek when eating and pain during sexual intercourse for the past week. She has not been sick for the past 6 months. She has started hiking in the woods on the weekends with her son a couple months ago but has been careful to avoid poison ivy. She has a history of hypertension and osteoarthritis. She recently started taking captopril and stopped taking meloxicam 2 weeks ago. She has a family history of pernicious anemia and Graves' disease. The patient's vital signs are within normal limits. Examination reveals multiple, flaccid blisters on the volar surface of the forearm and ulcers on the buccal, gingival, and vulvar mucosa. The epidermis on the forearm separates when the skin is lightly stroked. The total body surface area involvement of the blisters is estimated to be 10%. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?
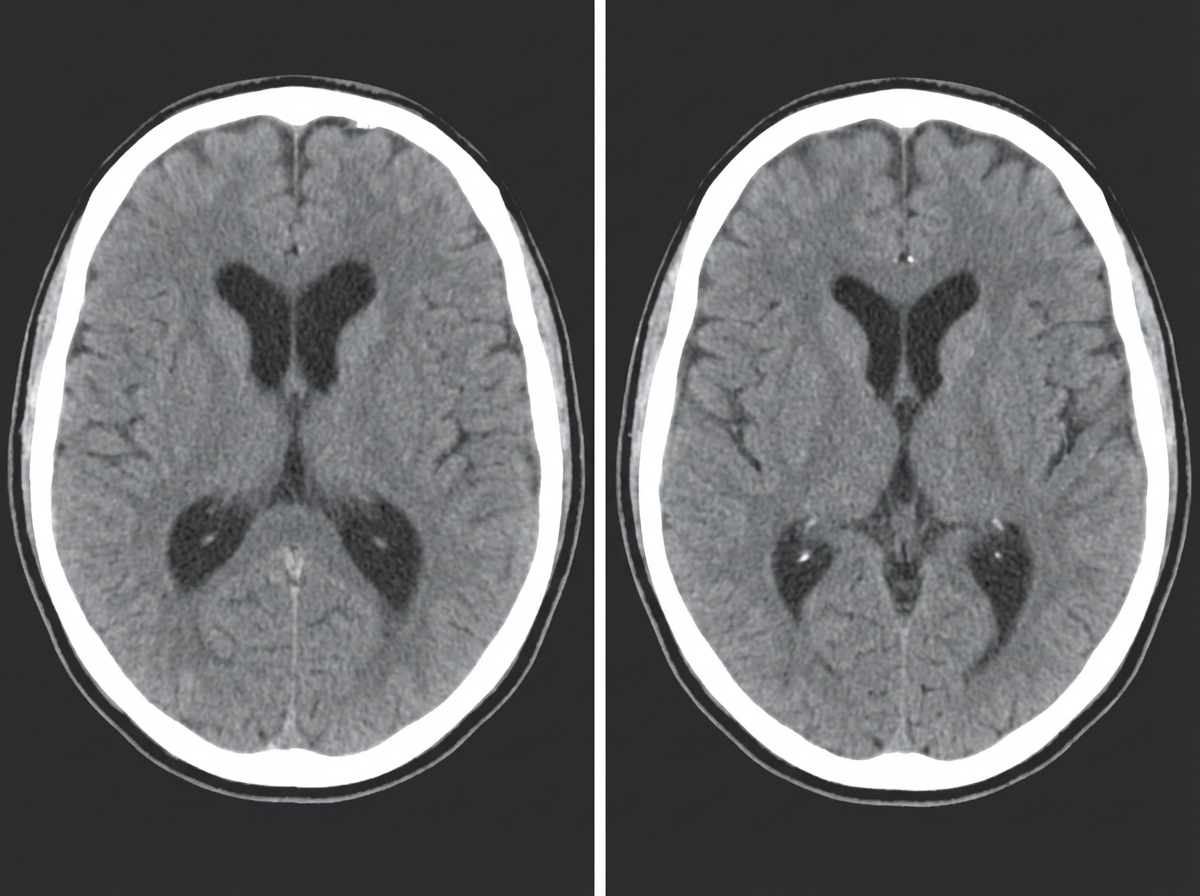
A 45-year-old man is brought by his wife with a complaint of an ongoing progressive history of memory problems for 6 months. He is an accountant by profession. He has difficulty remembering things and events, which has affected his job. He began using a diary to aid with remembering his agenda. His wife also says that he has wet his pants multiple times in the past 2 months and he avoids going out. He has been smoking 1 pack of cigarettes daily for the past 20 years. His past medical history is unremarkable. The vital signs include: blood pressure of 134/76 mm Hg, a pulse of 70 per minute, and a temperature of 37.0°C (98.6°F). His mini-mental state examination (MMSE) result is 22/30. His extraocular movements are normal. The muscle tone and strength are normal in all 4 limbs. The sensory examination is unremarkable. He has an absent Romberg's sign. He walks slowly, taking small steps, with feet wide apart as if his feet are stuck to the floor. The CT scan of the head is shown in the image. What is the most likely diagnosis of the patient?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app