
Differential diagnosis — MCQs

On this page
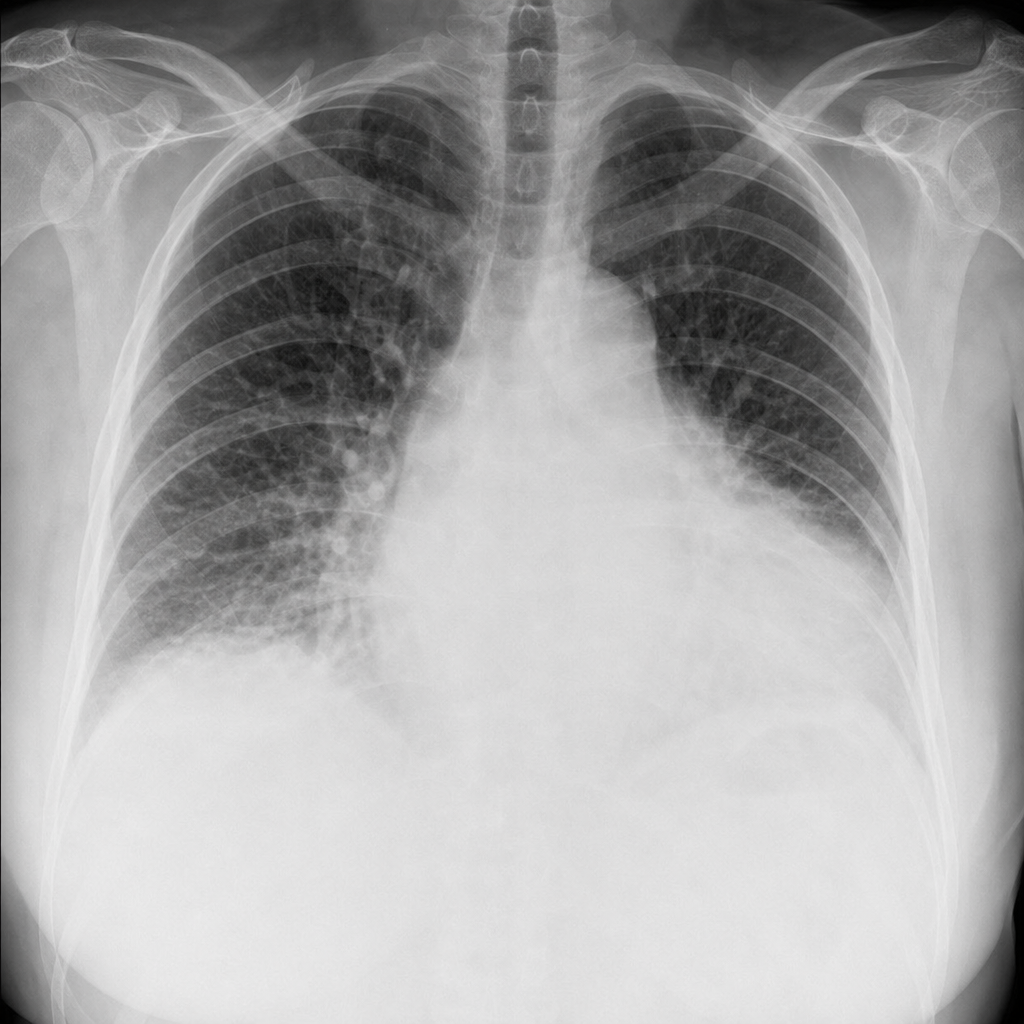
A 58-year-old woman presents with a 10-day history of progressively worsening exertional dyspnea and bilateral leg swelling. She has a history of hypertension treated with lisinopril for 6 years. She recently completed a 6-month course of doxorubicin-based chemotherapy for breast cancer, finishing 3 months ago. Temperature 37.0°C, blood pressure 148/92 mmHg, heart rate 102 bpm, oxygen saturation 91% on room air. JVP is elevated at 10 cm. Bibasilar crackles are present. An ECG shows sinus tachycardia with no ischemic changes. The chest radiograph image shown demonstrates the finding most critical to establishing the diagnosis. Which of the following is the most likely diagnosis?
A female presents with a 1 × 1 cm thyroid swelling. What is the next best step in management?
What is the most appropriate initial investigation for a solitary thyroid nodule (STN)?
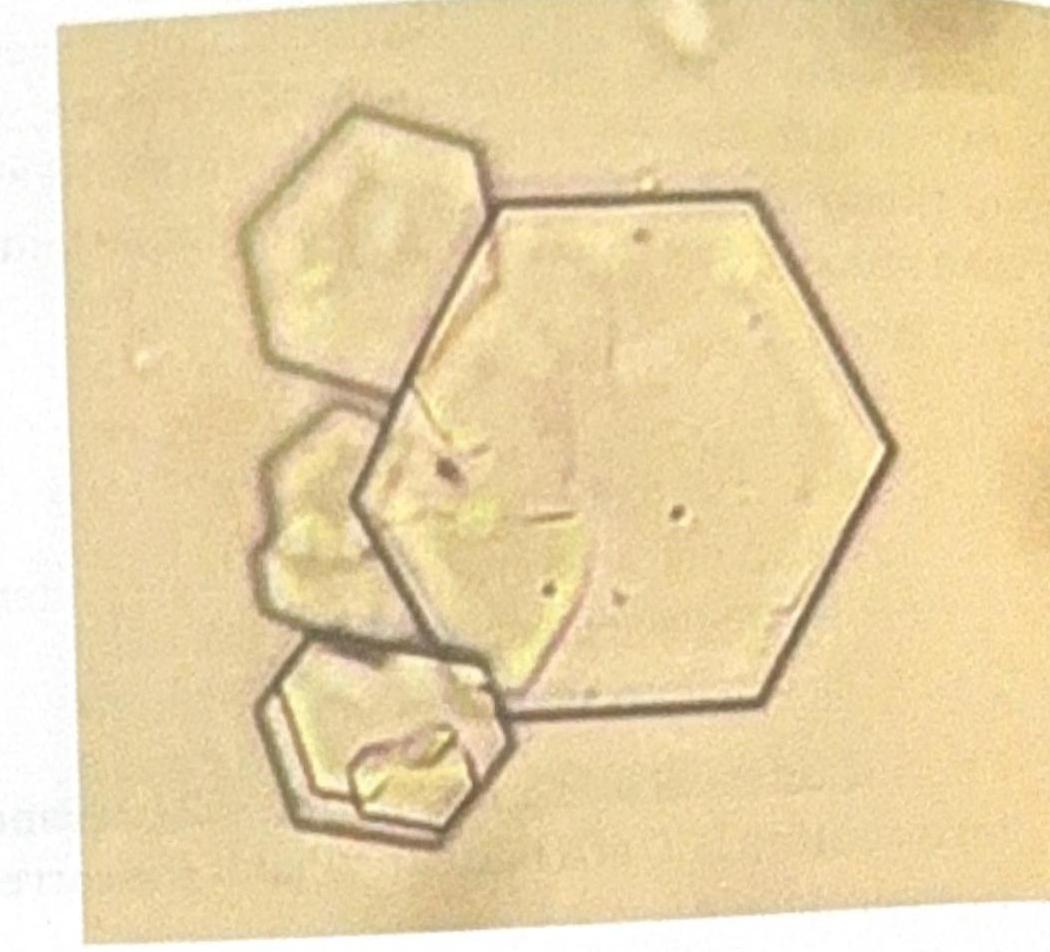
A young patient presents to the OPD with recurrent colicky abdominal pain. Urine examination shows the presence of red blood cells (RBCs) and the following crystal shape in the figure. What is the most likely diagnosis?
An 11-year-old boy is brought to the emergency department 30 minutes after he was found screaming and clutching his head. He has had nausea and occasional episodes of vomiting for 1 week, fever and left-sided headaches for 2 weeks, and increasing tooth pain over the past 3 weeks. He has no history of ear or sinus infections. He is in moderate distress. His temperature is 38.7°C (101.7°F), pulse is 170/min, respirations are 19/min, and blood pressure is 122/85 mmHg. He is confused and only oriented to person. The pupils react sluggishly to light. Fundoscopic examination shows papilledema bilaterally. Extraocular movements are normal. Flexion of the neck causes hip flexion. Which of the following is the most likely diagnosis?
Practice by Chapter
Symptom-based differential diagnosis approach
Practice Questions
System-based differential construction
Practice Questions
Probability ranking in differentials
Practice Questions
Common vs rare disease considerations
Practice Questions
Age and demographic considerations
Practice Questions
Pattern recognition in diagnosis
Practice Questions
Anatomical approach to differential diagnosis
Practice Questions
Syndrome recognition
Practice Questions
Refinement of differential with testing
Practice Questions
Interpreting diagnostic ambiguity
Practice Questions
Ruling in vs ruling out strategies
Practice Questions
Cognitive biases in differential construction
Practice Questions
Integration of diagnostic information
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app