
Clinical Reasoning — MCQs

On this page
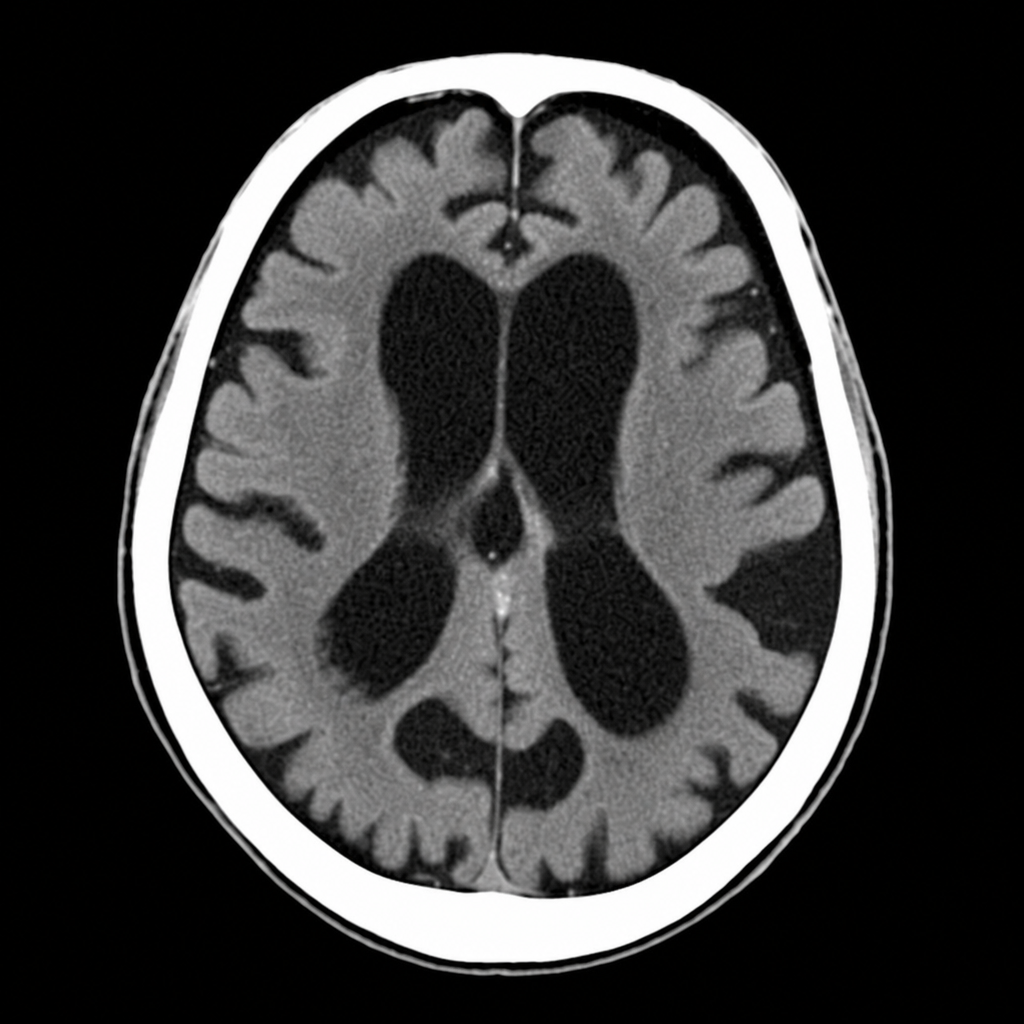
A 72-year-old woman is brought in by her daughter for progressive confusion over 4 weeks, 8 kg of unintentional weight loss over 3 months, and new-onset urinary incontinence. She has no history of psychiatric illness. Medications include amlodipine and aspirin. On examination, she is afebrile; she scores 19/30 on the MMSE. Gait is broad-based and magnetic in quality. Neurological exam shows no focal deficits and no papilledema. CBC, CMP, TSH, B12, and RPR are all within normal limits. The image shown is from her MRI brain. Which of the following diagnoses is most consistent with the clinical presentation and imaging finding?
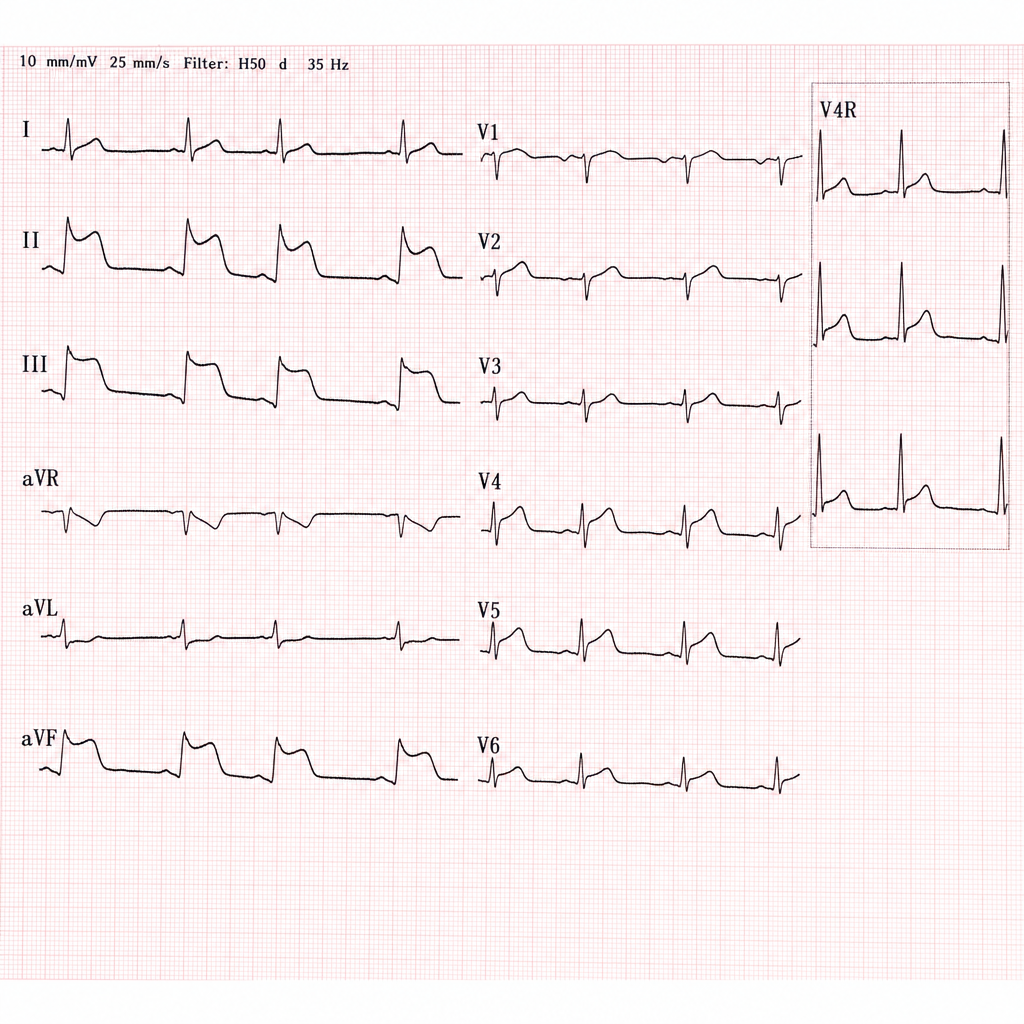
A 12-lead ECG with right-sided leads (including V4R) is shown for a 61-year-old man who presented with 40 minutes of crushing substernal chest pressure, diaphoresis, and nausea. His blood pressure is 88/60 mmHg and heart rate is 42 bpm. Lungs are clear to auscultation. Jugular venous distension is present. Based on the ECG findings, which diagnosis most precisely localizes the culprit lesion and accounts for the hemodynamic profile?
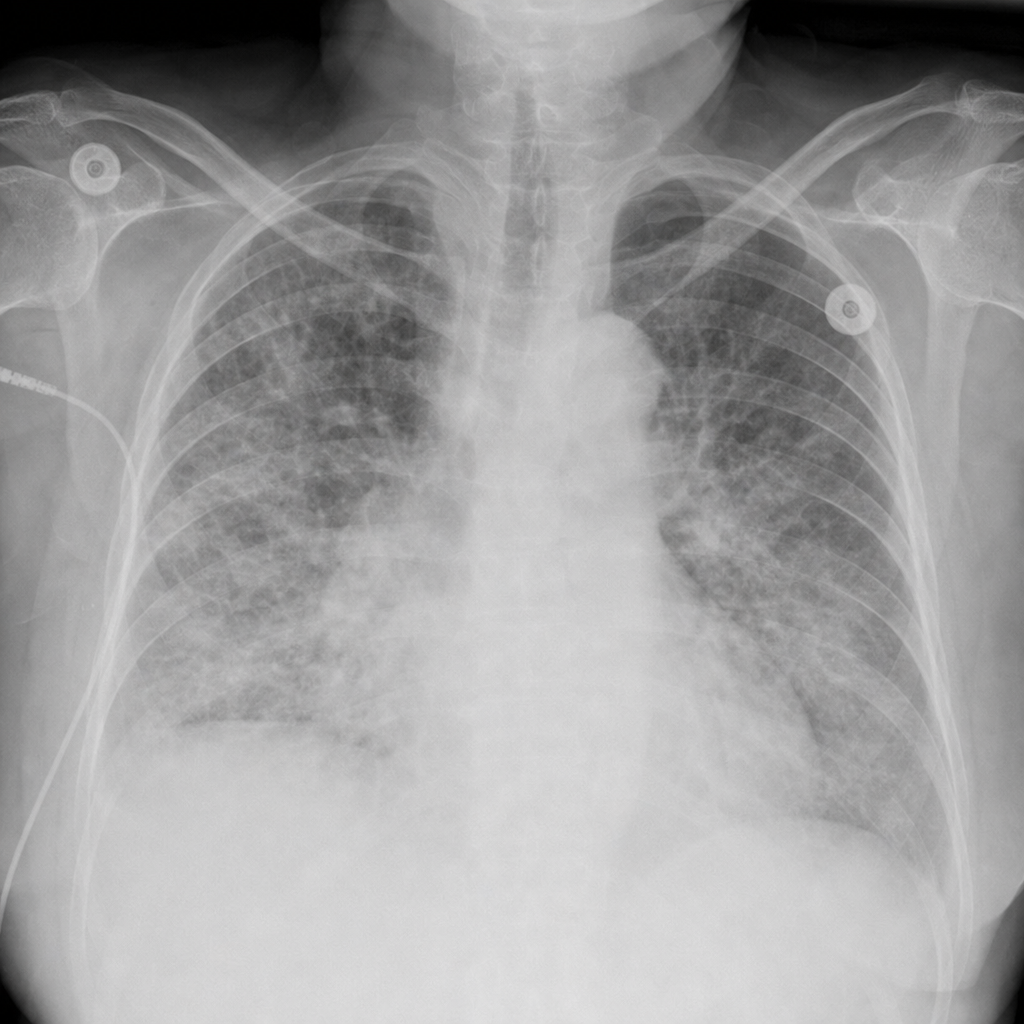
A 72-year-old immunocompromised woman receiving long-term corticosteroids for rheumatoid arthritis presents with a 5-day history of progressive dyspnea, non-productive cough, and low-grade fever. She denies rigors or purulent sputum. Oxygen saturation is 88% on room air. The image shown was obtained on presentation. Which diagnosis is most consistent with the radiographic pattern and clinical context?
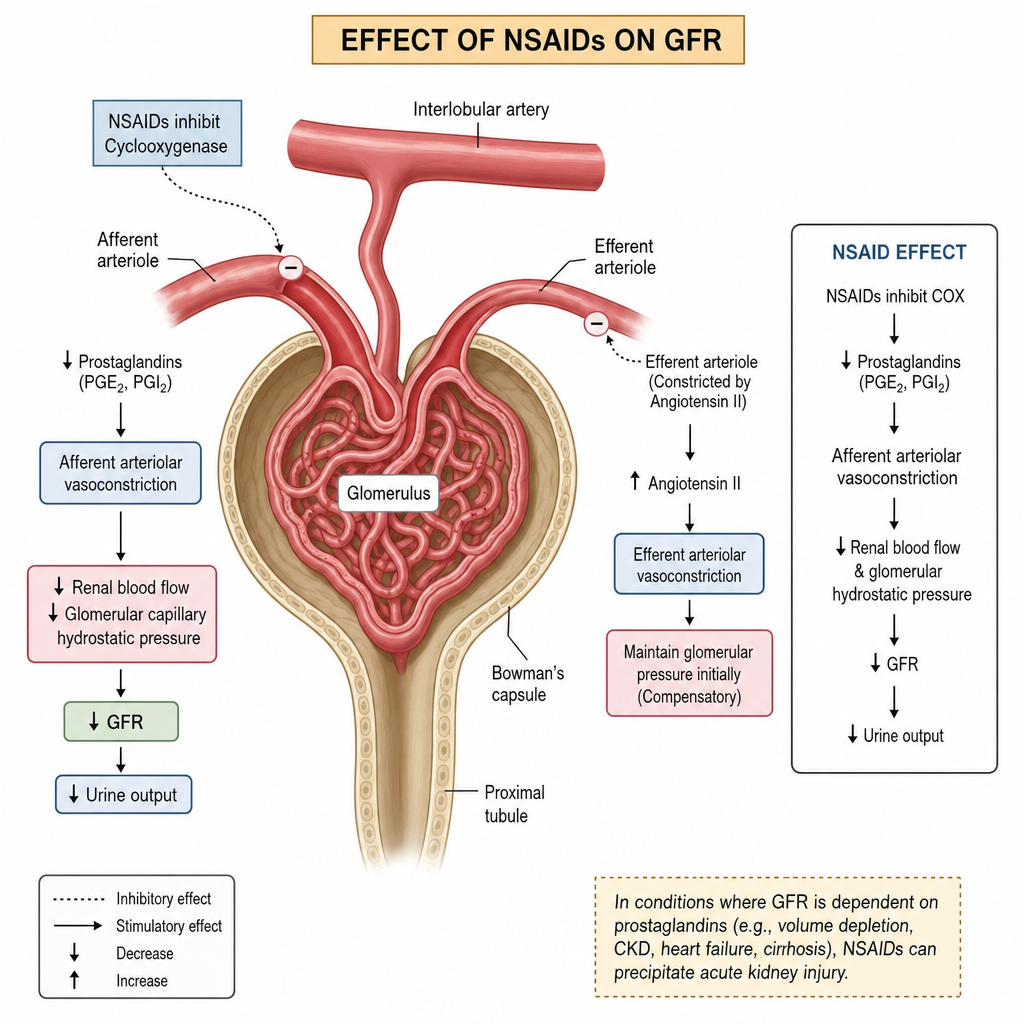
A 55-year-old man with type 2 diabetes and hypertension presents with a 2-day history of decreased urine output and bilateral leg swelling. He started ibuprofen 10 days ago for knee pain. Medications include metformin, lisinopril, and hydrochlorothiazide. Labs: serum creatinine 3.1 mg/dL (baseline 1.0 mg/dL), BUN 54 mg/dL, sodium 138 mEq/L, potassium 5.6 mEq/L. Urinalysis: specific gravity 1.010, no casts, trace protein. Urine sodium 48 mEq/L, urine creatinine 60 mg/dL. The image shown is a renal ultrasound obtained at the time of presentation. Which of the following is the most likely cause of this patient's acute kidney injury?
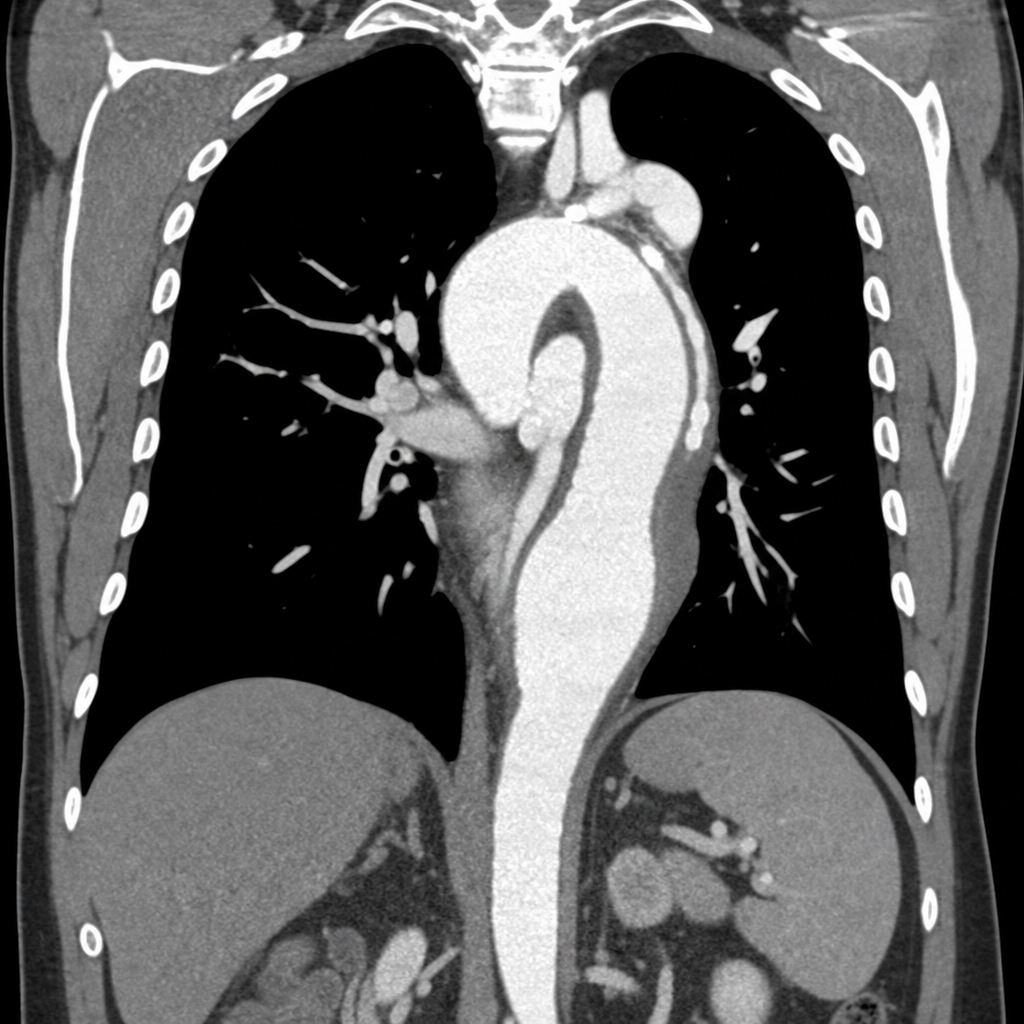
A 61-year-old man presents to the emergency department with sudden-onset severe chest pain radiating to his back, described as 'tearing,' with onset 90 minutes ago. He has a history of poorly controlled hypertension. BP is 178/96 mmHg in the right arm and 142/80 mmHg in the left arm. Heart rate is 102 bpm. He is hemodynamically stable. Auscultation reveals a soft early diastolic murmur at the left sternal border. ECG shows sinus tachycardia with left ventricular hypertrophy and no ST changes. The chest radiograph image shown is obtained. Based on the image finding combined with the clinical presentation, which of the following is the most appropriate next diagnostic step?
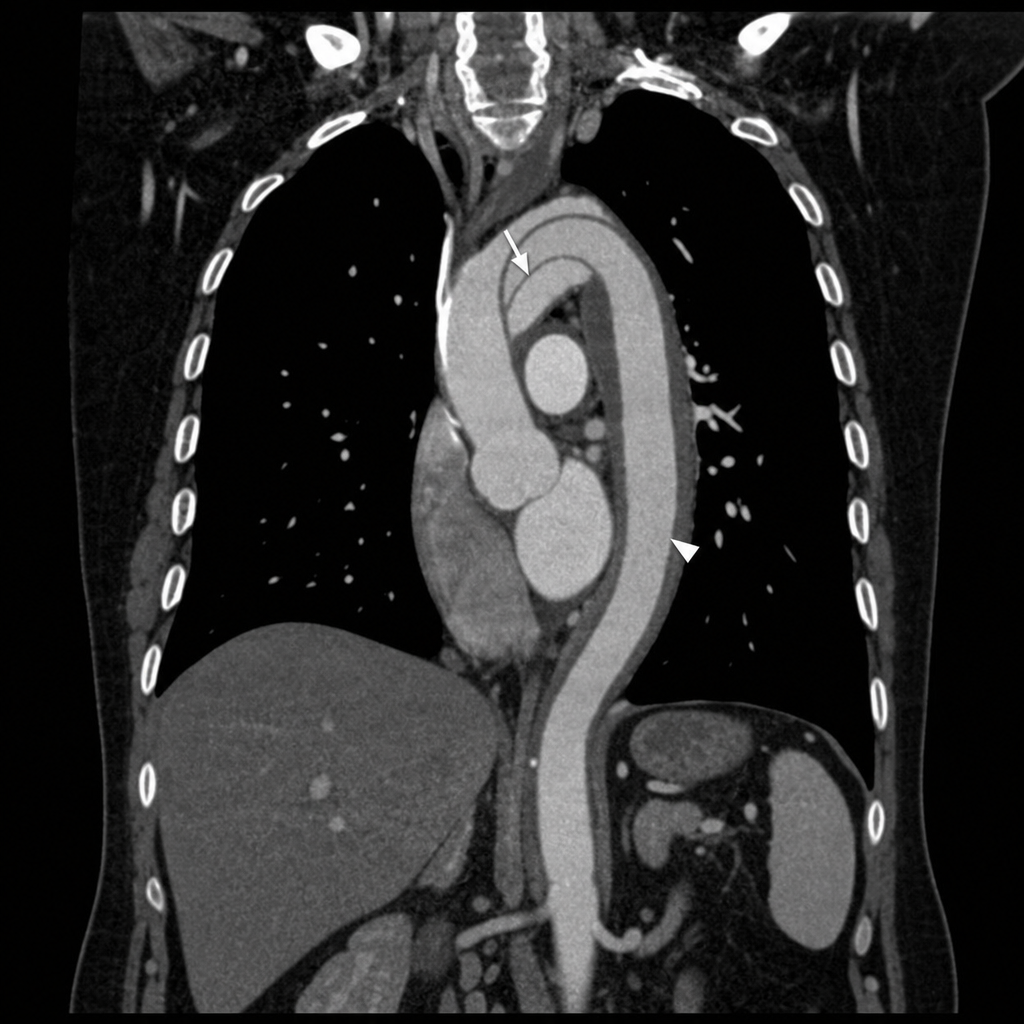
A 48-year-old man presents to the emergency department with sudden-onset tearing chest pain that radiates to his back and interscapular region. He describes the pain as 'the worst of his life,' beginning abruptly 2 hours ago. He has a history of poorly controlled hypertension and Marfan syndrome. On examination, blood pressure is 178/94 mmHg in the right arm and 142/80 mmHg in the left arm. Heart rate is 102 bpm. Aortic regurgitation murmur is heard. ECG shows sinus tachycardia with no ST changes. The chest radiograph image shown demonstrates a widened mediastinum with an indistinct aortic knob and rightward tracheal deviation. He is hemodynamically stable. Which of the following is the most appropriate next diagnostic step to confirm the suspected diagnosis?
A 53-year-old man presents with a 2-year-history of dull, nonspecific flank pain that subsides with rest. His past medical history is significant for hypertension, hypercholesterolemia, and type 2 diabetes mellitus. He has no allergies and takes no medications. His father died of kidney disease at the age of 51, and his mother has been treated for ovarian cancer. On presentation, his blood pressure is 168/98 mm Hg, and his heart rate is 102/min. Abdominal examination is significant for palpable bilateral renal masses. His laboratory tests are significant for creatinine of 2.0 mg/dL and a BUN of 22 mg/dL. Which of the following tests is most recommended in this patient?
A 50-year-old woman presents with severe abdominal pain. Past medical history is significant for a peptic ulcer. Physical examination is limited because the patient will not allow abdominal palpation due to the pain. The attending makes a presumptive diagnosis of peritonitis. Which of the following non-invasive maneuvers would be most helpful in confirming the diagnosis of peritonitis in this patient?
A 63-year-old retired teacher presents to his family physician for an annual visit. He has been healthy for most of his life and currently takes no medications, although he has had elevated blood pressure on several visits in the past few years but declined taking any medication. He has no complaints about his health and has been enjoying time with his grandchildren. He has been a smoker for 40 years–ranging from half to 1 pack a day, and he drinks 1 beer daily. On presentation, his blood pressure is 151/98 mm Hg in both arms, heart rate is 89/min, and respiratory rate is 14/min. Physical examination reveals a well-appearing man with no physical abnormalities. A urinalysis is performed and shows microscopic hematuria. Which of the following is the best next step for this patient?
A 73-year-old man comes to the physician because of a 4-kg (9-lb) weight loss over the last month. During this time he has not been able to eat more than one bite without coughing immediately and sometimes he regurgitates food through his nose. His symptoms are worse with liquids. One month ago he had a stroke in the right middle cerebral artery. He has a history of hypertension, type 2 diabetes mellitus, and hyperlipidemia. Current medications include aspirin, amlodipine, metformin, and simvastatin. Examination of the oropharynx, chest, and abdomen shows no abnormalities. Neurological examination shows facial drooping on the left and decreased strength in the left upper and lower extremities. Which of the following is the most appropriate next step in management?
Practice by Chapter
Analytical vs non-analytical reasoning
Practice Questions
Hypothetico-deductive reasoning
Practice Questions
Pattern recognition in clinical reasoning
Practice Questions
Probabilistic reasoning
Practice Questions
Bayesian approach to diagnosis
Practice Questions
Decision making under uncertainty
Practice Questions
Cognitive biases in clinical reasoning
Practice Questions
Metacognition and diagnostic calibration
Practice Questions
Clinical decision rules
Practice Questions
Diagnostic parsimony (Occam's razor)
Practice Questions
Diagnostic thoroughness (Hickam's dictum)
Practice Questions
Diagnostic error analysis
Practice Questions
Integrating evidence-based medicine into reasoning
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app