
Airway, Breathing, Circulation priorities — MCQs

A 45-year-old man was a driver in a motor vehicle collision. The patient is not able to offer a medical history during initial presentation. His temperature is 97.6°F (36.4°C), blood pressure is 104/74 mmHg, pulse is 150/min, respirations are 12/min, and oxygen saturation is 98% on room air. On exam, he does not open his eyes, he withdraws to pain, and he makes incomprehensible sounds. He has obvious signs of trauma to the chest and abdomen. His abdomen is distended and markedly tender to palpation. He also has an obvious open deformity of the left femur. What is the best initial step in management?
A 47-year-old man is brought to the emergency room by his wife. She states that they were having dinner at a restaurant when the patient suddenly became out of breath. His past medical history is irrelevant but has a 20-year pack smoking history. On evaluation, the patient is alert and verbally responsive but in moderate respiratory distress. His temperature is 37°C (98.6°F), blood pressure is 85/56 mm Hg, pulse is 102/min, and respirations are 20/min. His oxygen saturation is 88% on 2L nasal cannula. An oropharyngeal examination is unremarkable. The trachea is deviated to the left. Cardiopulmonary examination reveals decreased breath sounds on the right lower lung field with nondistended neck veins. Which of the following is the next best step in the management of this patient?
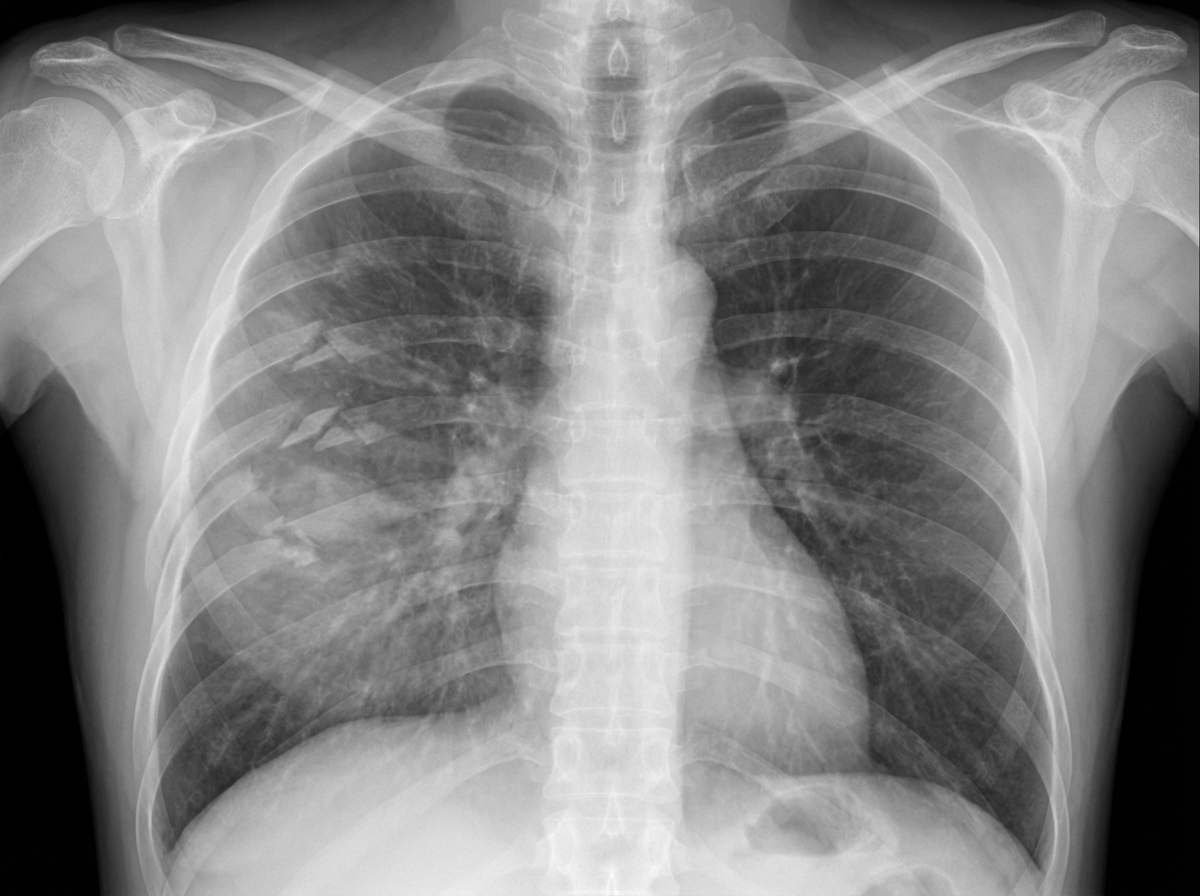
A 27-year-old man is brought to the emergency department 45 minutes after being involved in a motor vehicle collision. He is agitated. He has pain in his upper right arm, which he is cradling in his left arm. His temperature is 36.7°C (98°F), pulse is 135/min, respirations are 25/min, and blood pressure is 145/90 mm Hg. His breathing is shallow. Pulse oximetry on 100% oxygen via a non-rebreather face mask shows an oxygen saturation of 83%. He is confused and oriented only to person. Examination shows multiple bruises on the right anterior thoracic wall. The pupils are equal and reactive to light. On inspiration, his right chest wall demonstrates paradoxical inward movement while his left chest wall is expanding. There is pain to palpation and crepitus over his right anterior ribs. The remainder of the examination shows no abnormalities. An x-ray of the chest is shown. Two large-bore IVs are placed. After fluid resuscitation and analgesia, which of the following is the most appropriate next step in management?
A 28-year-old soldier is brought back to a military treatment facility 45 minutes after sustaining injuries in a building fire from a mortar attack. He was trapped inside the building for around 20 minutes. On arrival, he is confused and appears uncomfortable. He has a Glasgow Coma Score of 13. His pulse is 113/min, respirations are 18/min, and blood pressure is 108/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. Examination shows multiple second-degree burns over the chest and bilateral upper extremities and third-degree burns over the face. There are black sediments seen within the nose and mouth. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. Intravenous fluid resuscitation is begun. Which of the following is the most appropriate next step in management?
A 15-year-old boy is brought to the emergency department one hour after sustaining an injury during football practice. He collided head-on into another player while wearing a mouthguard and helmet. Immediately after the collision he was confused but able to use appropriate words. He opened his eyes spontaneously and followed commands. There was no loss of consciousness. He also had a headache with dizziness and nausea. He is no longer confused upon arrival. He feels well. Vital signs are within normal limits. He is fully alert and oriented. His speech is organized and he is able to perform tasks demonstrating full attention, memory, and balance. Neurological examination shows no abnormalities. There is mild tenderness to palpation over the crown of his head but no signs of skin break or fracture. Which of the following is the most appropriate next step?
A 27-year-old soldier stationed in Libya sustains a shrapnel injury during an attack, causing a traumatic above-elbow amputation. The resulting arterial bleed is managed with a tourniquet prior to transport to the military treatment facility. On arrival, he is alert and oriented to person, place, and time. His armor and clothing are removed. His pulse is 145/min, respirations are 28/min, and blood pressure is 95/52 mm Hg. Pulmonary examination shows symmetric chest rise. The lungs are clear to auscultation. Abdominal examination shows no abnormalities. There are multiple shrapnel wounds over the upper and lower extremities. A tourniquet is in place around the right upper extremity; the right proximal forearm has been amputated. One large-bore intravenous catheter is placed in the left antecubital fossa. Despite multiple attempts, medical staff is unable to establish additional intravenous access. Which of the following is the most appropriate next step in management?
A 17-year-old boy is brought to the emergency department by his parents 6 hours after he suddenly began to experience dyspnea and pleuritic chest pain at home. He has a remote history of asthma in childhood but has not required any treatment since the age of four. His temperature is 98.4°F (36.9°C), blood pressure is 100/76 mmHg, pulse is 125/min, respirations are 24/min. On exam, he has decreased lung sounds and hyperresonance in the left upper lung field. A chest radiograph shows a slight tracheal shift to the right. What is the best next step in management?
A 57-year-old man was brought into the emergency department unconscious 2 days ago. His friends who were with him at that time say he collapsed on the street. Upon arrival to the ED, he had a generalized tonic seizure. At that time, he was intubated and is being treated with diazepam and phenytoin. A noncontrast head CT revealed hemorrhages within the pons and cerebellum with a mass effect and tonsillar herniation. Today, his blood pressure is 110/65 mm Hg, heart rate is 65/min, respiratory rate is 12/min (intubated, ventilator settings: tidal volume (TV) 600 ml, positive end-expiratory pressure (PEEP) 5 cm H2O, and FiO2 40%), and temperature is 37.0°C (98.6°F). On physical examination, the patient is in a comatose state. Pupils are 4 mm bilaterally and unresponsive to light. Cornea reflexes are absent. Gag reflex and cough reflex are also absent. Which of the following is the next best step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app